Three Teams. One Mission. A First-of-Its-Kind Virtual Care Model
CHARLESTON, S.C., June 2, 2026 – Anuvia Prevention & Recovery Center, VirtuAlly, and AvaSure have successfully launched a purpose-built virtual nursing program designed specifically for the unique clinical environment of substance use and behavioral health treatment.
Substance use and residential behavioral health programs face the same nationwide nursing shortages as acute care, often with fewer resources and tighter regulatory oversight. This virtual nursing program extends access to experienced nurses 24/7, strengthening client safety, supporting regulatory compliance, and enabling cost-effective care delivery without expanding on-site staffing.
This go-live marks a first: a virtual care model intentionally designed for a residential treatment setting, where client complexity, strict regulatory requirements, and the realities of a nonprofit healthcare environment demand far more than an off-the-shelf approach.
Anuvia, a CARF-accredited nonprofit serving the Charlotte, North Carolina region, provides a comprehensive continuum of substance use disorder and behavioral health treatment for adults, adolescents, and veterans. Services include residential treatment with withdrawal management, medication-assisted treatment (MAT), medication management, outpatient programs for substance use disorder and mental health services, and community-based behavioral healthcare. Integrating virtual nursing into an environment like Anuvia’s required all three organizations to think differently, collaborate closely, and address challenges that had not previously been encountered in this type of care setting.
Why This Setting Is Different
Acute hospital virtual nursing programs are becoming increasingly common. But Anuvia is not a hospital, and that distinction matters.
Substance use treatment facilities operate under a different regulatory framework. In North Carolina, residential programs are governed by stringent state guidelines and accredited by CARF (Commission on Accreditation of Rehabilitation Facilities), an internationally recognized accreditor for health and human services organizations. Individuals served at Anuvia are navigating complex physical and emotional recovery journeys that often involve substance use and behavioral health treatment, medication-assisted treatment, and management of chronic physical and behavioral health needs. The care provided must be highly individualized, relationship-centered, and designed to support long-term wellness and recovery.
Deploying virtual nursing in this environment required rethinking workflows, redefining how on-site and virtual teams collaborate, and building clinical processes with regulatory compliance embedded from the start. Not retrofitted later.
It also required a cost-conscious approach. As a nonprofit, Anuvia is committed to directing resources toward client care. Virtual nursing created a path to strengthen clinical support without expanding in-house staffing, but only if the model was designed with that reality in mind.
How the Three Teams Built Something New
The foundation for this program was established before any technology was selected.
VirtuAlly’s clinical and implementation teams worked alongside Anuvia’s leadership and frontline staff to understand the problem before designing the solution. This included assessing staffing realities; mapping nursing use cases specific to residential substance use treatment; identifying workflow gaps; and defining the clinical, operational, and compliance requirements that guided every decision.
AvaSure was selected as the virtual care platform partner for this deployment, bringing a scalable, enterprise-ready foundation. By leveraging an established technology platform and aligning it with VirtuAlly’s clinical workflows and program design, the teams were able to accelerate deployment without starting from scratch. Together, VirtuAlly’s clinical expertise and AvaSure’s platform enabled a solution tailored to Anuvia’s environment.
The result is a virtual nursing model that supports 24/7 clinical availability across three critical functions:
Admission Screening of Clients: VirtuAlly nurses provide around-the-clock screening to ensure individuals are medically appropriate for admission before entering the residential program.
Medication Review at Admission: During admission, virtual nurses review and verify client-provided medications to support accurate documentation and ensure individuals enter the program with a clear and complete medication profile.
Triage of Acute Medical Need: When urgent clinical situations arise, VirtuAlly nurses provide immediate virtual triage support, extending the clinical decision-making capacity of Anuvia’s on-site team at any hour.
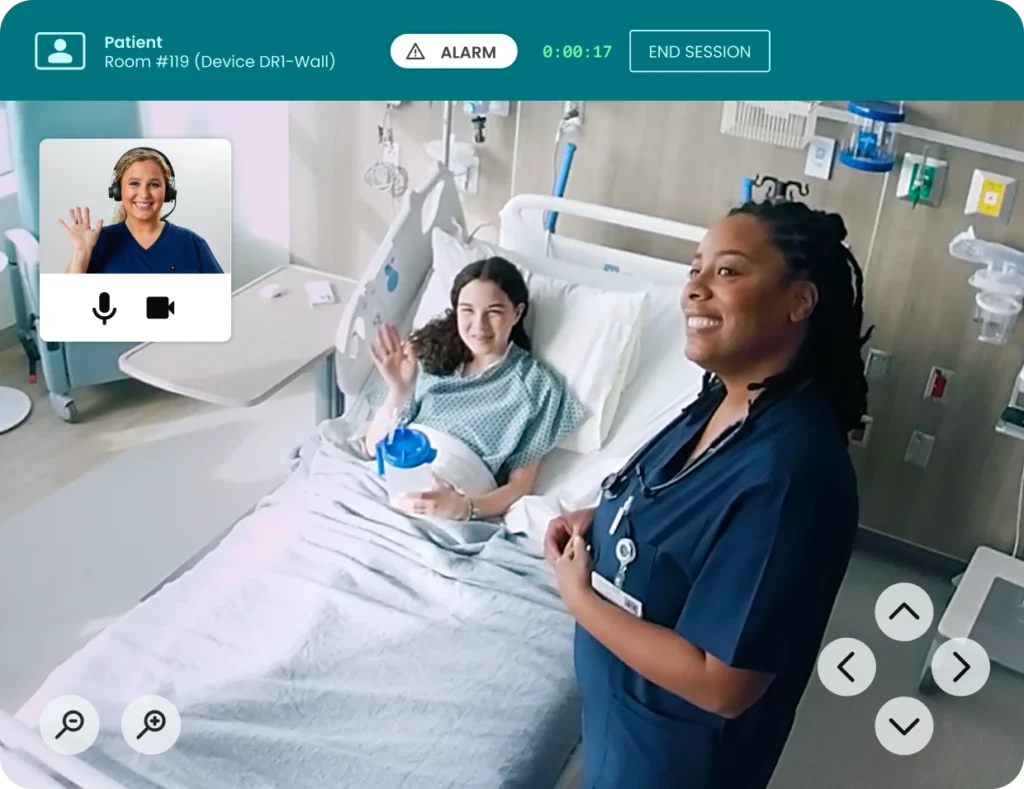
AvaSure’s virtual care and smart room platform enables real-time clinical intervention through two-way virtual care devices and virtual visit capabilities, alongside continuous observation, AI-powered fall prevention, and elopement detection.
One standout innovation developed through this collaboration is virtual medication verification. VirtuAlly nurses support on-site staff by reviewing client-provided, home medications, helping ensure everyone arrives with the medications needed for a successful treatment stay. This process focuses on medication inventory and documentation, supporting accuracy and continuity of care.
Throughout implementation, VirtuAlly also provided consultative support beyond standard deployment, helping Anuvia navigate program changes, adapt to evolving service definitions, and ensure workflows align with the expectations of the North Carolina Board of Nursing, CARF, and state oversight bodies.
Looking Ahead
“Behavioral health and addiction treatment has been underserved by virtual care for too long. What we built with Anuvia and AvaSure proves that a clinically rigorous, purpose-built virtual nursing model works in this setting. That matters for Anuvia’s clients today, and for every organization in this space wondering if it’s possible.”— Joe Weschler, CEO, VirtuAlly
“Anuvia’s approach to bringing together the right solutions to address a complex challenge demonstrates how innovation and outcomes must go hand in hand. By aligning technology with a clearly defined care model, they’ve improved client safety, enhanced quality of care, supported their teams, and increased operational efficiency. This is the future of virtual care. Scalable solutions that deliver both clinical impact and economic value.” — Adam McMullin, CEO, AvaSure
VirtuAlly’s customer success team remains actively engaged with Anuvia to refine workflows, evolve service delivery, and build toward measurable outcomes in client safety and care quality. As the program matures, all three organizations plan to share learnings that can help inform how the broader behavioral health and addiction treatment sector approaches virtual care.
The work at Anuvia is a proof point, not a ceiling. As virtual care continues to expand beyond acute settings, this program offers a replicable model for behavioral health and addiction treatment organizations looking to strengthen clinical capacity, meet regulatory standards, and deliver better outcomes for the people they serve.
About VirtuAlly
VirtuAlly is the virtual clinical care team built to extend the capabilities of bedside nurses, strengthen patient safety, and deliver outcomes that health systems can measure. Founded at MUSC, VirtuAlly is one of only three federally recognized Telehealth Centers of Excellence in the country and among the first virtual nursing organizations to achieve Joint Commission Accreditation. VirtuAlly delivers virtual nursing, telesitting, remote patient monitoring, and telemetry, purpose-built for the real demands of today’s care environment. To learn more, visit virtually.io.
VirtuAlly Media Contact: Megan Pino 412-999-2301 Mpino@virtually.io
About AvaSure
AvaSure® is an intelligent virtual care platform that healthcare providers use to engage with patients, optimize staffing, and seamlessly blend remote and in-person care at scale. The platform deploys AI-powered virtual sitting and virtual nursing solutions, meets the highest enterprise IT standards, and drives measurable outcomes with support from care experts. AvaSure consistently delivers a 6x ROI and has been recognized by KLAS Research as the #1 solution for reducing the cost of care. With a team of
15% nurses, AvaSure is a trusted partner of 1,200+ hospitals with experience in over 5,000 deployments. To learn more, visit www.avasure.com.
AvaSure Media Contact: Rachel Ford Hutman 301-801-5540 Rachel@fordhutmanmedia.com
Use Cases, Benefits, and Considerations for Hospitals
What is TeleSitter?
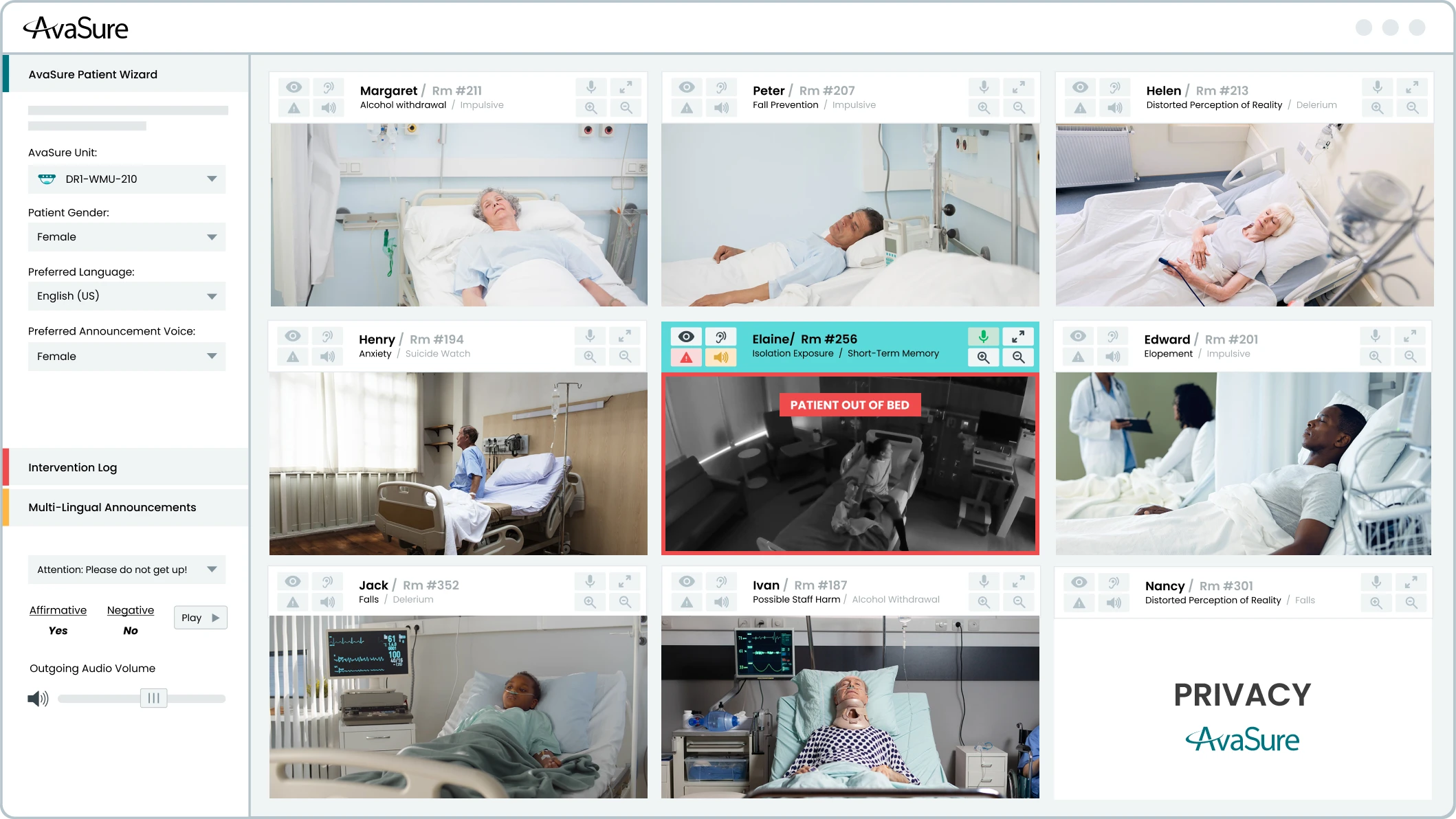
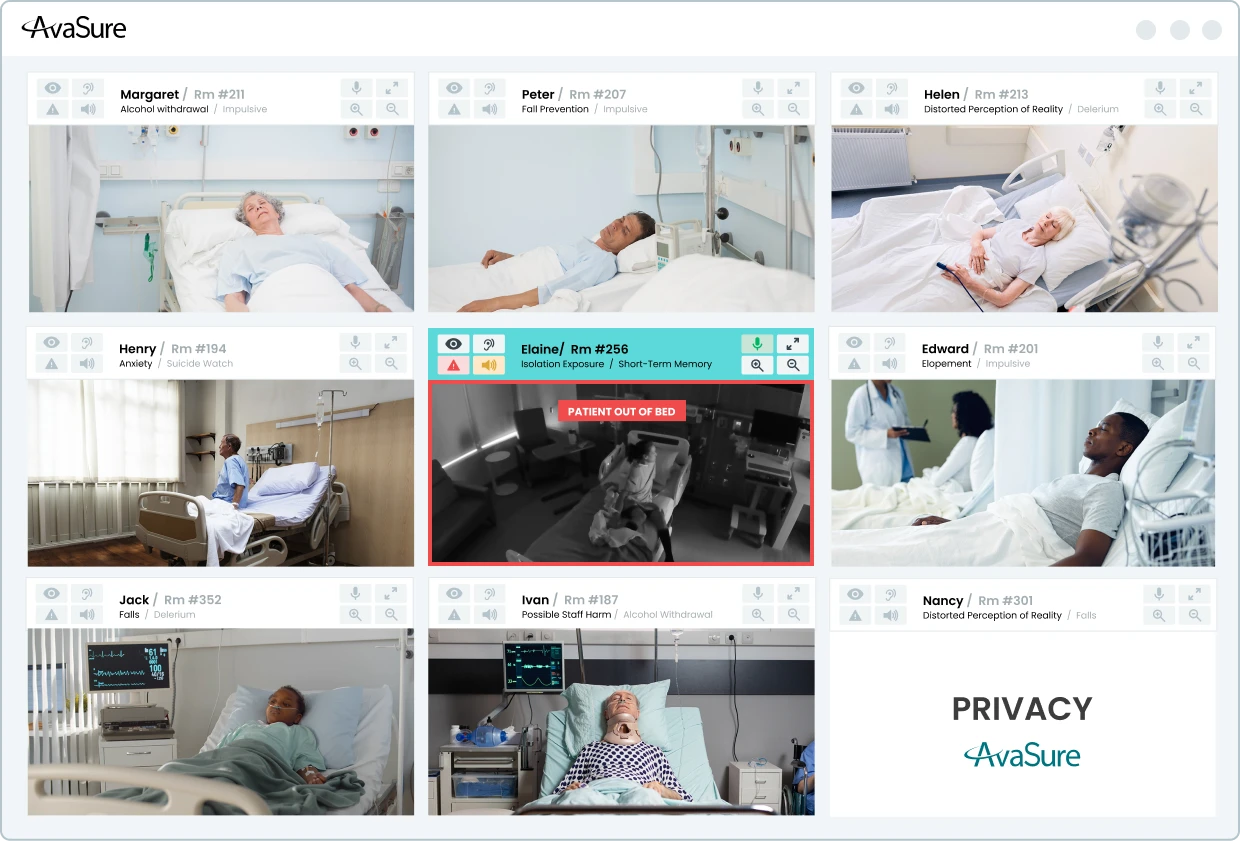
TeleSitter is a continuous remote patient monitoring platform used in hospitals that allows a single trained virtual safety attendant (VSA) to monitor multiple at-risk patients simultaneously. The VSA uses the solution to prevent patient falls and elopement, workplace violence, and behavioral health risks.
AvaSure invented the TeleSitter® solution in 2008, creating a category-defining remote patient observation technology designed to help hospitals reduce the cost and dependency of one-to-one bedside sitters while maintaining patient safety. The TeleSitter solution delivers a 6x ROI, reduces adverse events by over 50%, reduces reliance on 1:1 sitters by up to 90%, and brings nursing staff back to the bedside.
What does TeleSitter do?
TeleSitter enables a single virtual safety attendant to monitor multiple at-risk patients simultaneously on one screen to prevent falls, elopement, workplace violence, and behavioral health risks.
Common use cases for virtual sitting:
Fall Prevention
One of the most common use cases for TeleSitter is fall prevention. Virtual Safety Attendants use the TeleSitter application to monitor patients at risk of falls. If they see a patient getting out of bed or not listening to instructions, they can send automated voice commands, speak directly to the patient, or activate the stat alarm — a loud, audible alarm in the patient’s room — to alert bedside care team members that a patient needs immediate assistance. This alarm can be routed through nurse call, mobile devices, or dome light systems for immediate action. Hospitals using TeleSitter have documented fall rate reductions exceeding 50%, and one health system saved $3.2 million from sitter cost reductions and avoided fall-related costs, while another saved $1.5M in just one year. However, while keeping patients safe from falls is where this technology started, it’s only the beginning of what it can do.
Elopement Prevention
Elopement prevention is another one of the most common use cases of TeleSitter. Patients who are disoriented, cognitively impaired, or in a behavioral health crisis can move quickly, and by the time a bedside nurse notices something is wrong, precious time has already been lost. Virtual Safety Attendants and AI monitoring are trained to recognize the early behavioral cues that precede an elopement attempt — restlessness, repositioning, reaching for side rails — and intervene verbally before a patient ever gets to the door.
Workplace Violence Prevention
TeleSitter can also be used to prevent workplace violence. Healthcare workers face a disproportionately high risk of violence compared to workers in other industries, and placing a 1:1 sitter physically in the room of an agitated patient doesn’t always make that situation safer. Virtual monitoring allows staff to observe, de-escalate, and call for backup from a position that keeps everyone protected. For behavioral health patients more broadly, the ability to maintain a constant, calm, remote presence — one that can redirect without escalating — has proven to be a genuinely different kind of intervention than what a physical sitter can offer.
Low-to-Moderate Suicide Risk Monitoring
Suicide risk monitoring for patients assessed at low-to-moderate suicide risk is another use case for TeleSitter that has grown substantially and carries meaningful clinical backing. The Joint Commission has formally recognized video monitoring as an acceptable intervention for this patient group, which has given hospitals the confidence to deploy it more broadly across medical and emergency department settings. Research led by David Kroll, MD, of Brigham & Women’s Hospital in Boston, has shown that having a nursing assistant sitting in the room of a suicidal ideation patient is unproven in preventing self-harm. By contrast, use of the TeleSitter solution (now Continuous Observation) on suicide risk patients resulted in zero adverse events (Kroll, 2019). This initial study laid the foundation for The Joint Commission to deem virtual sitting an acceptable intervention for low and moderately suicidal patients.
Pediatric Patient Monitoring
TeleSitter can be used for pediatric patient monitoring through multiple use cases. Pediatric care presents its own unique set of scenarios — from adolescents hospitalized for eating disorders, where constant supervision during meals and bathroom visits is clinically necessary but enormously staff-intensive, to infants at risk of falls when exhausted parents doze off while holding them, to children with autism or developmental disabilities who require consistent, attentive oversight without the potential agitation that a stranger in the room can sometimes cause. In each of these cases, virtual sitting offers a way to maintain the standard of care without the staffing burden that would otherwise make it unsustainable.
Whether the goal is protecting a vulnerable patient, de-escalating a difficult situation, or giving an overstretched nursing team a little more capacity, virtual sitting has proven it belongs at the center of a modern patient safety strategy.
Benefits and limitations of TeleSitter
The benefits of virtual sitting are real and well-documented. The most straightforward case for virtual sitting is economic: replacing 1:1 bedside sitters with a model where a single Virtual Safety Attendant monitors up to 36 patients simultaneously dramatically changes the labor math. Decades of peer-reviewed research have established that virtual monitoring is not merely equivalent to in-person sitting — in several key areas, it has proven superior. For fall prevention, for suicide risk monitoring, and for workplace violence prevention, studies consistently show that the virtual model performs as well or better than traditional 1:1 observation, while also reducing the emotional and physical burden on nursing teams (The Evidence-Based Case for a Virtual Care Solution). Research published in the Western Journal of Nursing Research found that virtual sitting actively reduces nurse burnout, with bedside staff viewing virtual monitoring as a resource that supports them rather than adding to their workload. That’s a benefit that extends well beyond the patients being monitored.
One of the limitations of TeleSitter on its own is that it is inherently reactive and scope-limited. While TeleSitter focuses on surveillance and verbal intervention, it does little to address the broader staffing crisis, documentation burden, or clinical complexity driving nurse burnout and attrition. With burnout affecting 56% of the nursing workforce, health systems need more than a safety tool — they need a new model of care delivery.
That evolution is Virtual Nursing, which extends the same trusted in-room device beyond observation to support admissions, discharges, medication reconciliation, patient and family education, rounding, specialty consults, and novice nurse mentorship — all without switching platforms or disrupting existing workflows. Rather than simply watching patients, Virtual Nurses now actively offload documentation burden, close the experience gap created by staffing shortages, and help systems achieve measurable clinical and financial ROI.
How TeleSitter solutions have evolved
Virtual care has expanded far beyond just virtual sitting. Thousands of health systems around the US have adopted full virtual care programs, where virtual sitting, virtual nursing, and AI workflows come together on one singular platform to streamline clinical workflows and enhance nurse and patient safety.
AvaSure has evolved far beyond its origins as the TeleSitter solution to become a comprehensive, AI-augmented Intelligent Virtual Care Platform trusted by more than 1,200 hospitals. The solution originally known as TeleSitter® is now called Continuous Observation, a name that better captures the platform’s modern capabilities: a single Virtual Safety Attendant monitoring up to 36 patients simultaneously, supported by ambient AI that detects potential adverse events before they occur. What began as a tool for remote patient safety monitoring has expanded into a unified platform supporting virtual sitting, virtual nursing, episodic consults, specialty care, and ambient AI — all running concurrently on a single in-room device. The Guardian DualFlex exemplifies this evolution: its dual-camera design pairs a 30x optical zoom PTZ camera for clinical workflows with a dedicated fixed wide-angle camera for AI, ensuring uninterrupted computer vision even during active patient consults. Five integrated microphones support ambient listening, voice command workflows, and future AI audio applications — all from one device mounted to the TV, wall, or ceiling. AvaSure’s open Partner API further extends the platform’s reach, enabling approved third-party ambient AI applications (such as Suki and Abridge for clinical documentation) to access device audio securely and write structured notes back to Epic1 flowsheets, without manual entry. AvaSure proudly holds Epic’s Inpatient Virtual Care Toolbox designation.
AvaSure continues to build the smart room of the future through purpose-built devices, an expanding AI platform developed, and deep EHR integration that makes virtual care a seamless, intelligent part of every patient interaction.
Contact AvaSure to learn more about how our virtual care platform can help keep both your patients and nurses safe.
The most common use cases for virtual sitting are fall prevention, elopement prevention, behavioral health monitoring, low to moderate suicide risk, workplace violence prevention, pediatric safety, isolation/infection prevention, pre-surgical monitoring and seizure monitoring.
The TeleSitter® solution delivers a 6x ROI, reduces adverse events by over 50%, and reduces reliance on 1:1 bedside sitters by over 75% — returning nursing staff to the bedside and alleviating burnout.
Peer-reviewed research consistently shows that virtual monitoring performs as well as — or better than — traditional 1:1 observation for fall prevention, suicide risk monitoring, and workplace violence prevention, while also reducing emotional and physical burden on nursing teams.
AvaSure has expanded well beyond its TeleSitter origins, evolving into a comprehensive Intelligent Virtual Care Platform deployed across more than 1,200 hospitals, supporting Continuous Observation, virtual nursing, episodic consults, specialty care, and ambient AI — all on a single platform.
AvaSure and Apella partner to deliver purpose-built ambient intelligence across the enterprise – helping hospitals avoid the compromises of one-size-fits-all platforms.
Hospitals are under increasing pressure to improve throughput, support overstretched care teams, and deliver measurable operational and financial outcomes amid rising costs, reduced reimbursement, and staffing challenges.
That is why AvaSure and Apella have formed a strategic alliance to bring connected ambient intelligence across the hospital – from inpatient care environments to the operating room.
AvaSure delivers one of the most widely adopted virtual care, ambient AI, and smart room platforms designed to optimize inpatient workflows, reduce costs, and expand access to care, while Apella provides real-time perioperative intelligence that helps surgical teams improve OR utilization, reduce delays, and optimize procedural flow with measurable operational and financial impact.
Together, the partnership helps hospitals improve throughput, coordination, and operational performance across the enterprise.
“Health systems are looking for technology investments that deliver measurable operational and financial value. By bringing together AvaSure’s virtual care platform and Apella’s perioperative intelligence capabilities, we are helping hospitals improve efficiency across critical care environments while driving verifiable financial and clinical outcomes – creating a stronger foundation for enterprise-wide operational transformation.” — Adam McMullin
Helping Hospitals Improve Operational and Financial Performance
Operational inefficiencies across inpatient and perioperative environments can have a significant impact on hospital capacity, staffing, and financial performance. Delays in patient progression, underutilized OR time, fragmented workflows, and administrative burden all contribute to rising costs and operational friction.
“Together, Apella and AvaSure deliver what most hospitals prioritize when it comes to their investments in modern AI: real operational ROI. Novel, trustworthy data is the starting point to delivering better outcomes for patients and care teams alike. Apella and AvaSure have collectively built the specialized expertise needed to optimize workflows across the entire surgical, pre-op, and post-op lifecycle.” — Jordan Tuttle, Apella Co-Founder and COO
Together, AvaSure and Apella help hospitals create greater operational visibility and workflow intelligence across the enterprise — enabling teams to improve throughput, optimize existing resources, and contribute to their bottom line.
Driving Operational Performance Across the Hospital
Through virtual care workflows, AvaSure helps health systems accelerate patient progression, streamline care coordination, and improve inpatient throughput. Apella extends real-time operational intelligence into the perioperative environment, helping surgical teams improve scheduling accuracy, reduce delays, and optimize OR utilization.
Organizations using AvaSure have achieved:
11.6% reduction in length of stay
16% reduction in ED holding time
31% reduction in discharge turnaround time
Organizations leveraging Apella have achieved:
24% improvement in scheduling accuracy
69-minute average reduction in surgical delays
56 additional block hours per OR, per month
Delivering Measurable Financial Impact
By helping hospitals optimize workflows and make better use of existing staff and capacity, both organizations are driving measurable financial outcomes.
At Houston Methodist, Apella helped generate approximately $2.2 million in additional revenue during a pilot focused on improving surgical block utilization and OR efficiency.
Meanwhile, Hackensack Meridian Health achieved approximately $1.6 million in cost savings through AvaSure virtual care initiatives driven by nurse retention improvements, reduced agency spend, length of stay improvements, readmission reductions, falls prevention, and reductions in CLABSI and CAUTI events.
In addition, AvaSure virtual sitter programs have helped health systems save more than $826 million in labor costs. And hospitals using Apella increase capacity for two more surgical cases per OR per month without the cost of additional facilities, staff, or overtime.
Purpose-Built Intelligence for High-Impact Care Environments
As health systems evaluate AI strategies, many are recognizing that different care environments require different operational workflows, data models, and intelligence capabilities.
Rather than forcing hospitals into generalized platforms designed to approach every environment the same way, AvaSure and Apella bring specialized intelligence to the areas where operational coordination, workflow efficiency, and resource optimization matter most.
By combining intelligent virtual care with AI-driven perioperative workflow intelligence, the partnership helps hospitals extend ambient intelligence across the enterprise while supporting the unique operational needs of both inpatient and surgical environments.
The Rural Health Transformation Program (RHTP) provides $50B in CMS funding (2026–2030) to strengthen rural hospitals.
States submitted transformation plans prioritizing technology, workforce resilience, and AI.
Virtual nursing, TeleHealth, and tele-specialty consults directly align with RHTP goals.
Hospitals can use RHTP funds to reduce falls, overtime, sitter costs, and specialty care gaps.
Sustainable virtual care models reinvest efficiency savings beyond federal funding.
What is the Rural Health Transformation Program (RHTP)?
Rural and community hospitals face critical workforce shortages and financial distress, with nearly half operating at a loss as of 2023, according to an AHA analysis of RAND Hospital Cost data. To address these pressures and improve care quality, Congress established theRural Health Transformation Program (RHTP)under the 2025 One Big Beautiful Bill Act (OBBBA). This $50 billion Centers for Medicare & Medicaid Services (CMS) initiative (FY 2026–2030) provides $10 billion annually to strengthen rural healthcare and offset projected funding gaps.
How CMS Administers RHTP Funding
States are the direct recipients and had to submit a Rural Health Transformation Plan for CMS approval. Half of the funding is divided equally among participating states—guaranteeing at least $100 million per year for five years if all states join—while the other half is distributed via a CMS formula. This massive pool supports infrastructure, technology, and workforce improvements for nearly 1,800 rural hospitals and 60 million residents.
How Critical Access Hospitals (CAHs) Benefit from RHTP Funding
While all rural providers are eligible, the nation’s 1,350 Critical Access Hospitals (CAHs) stand to benefit most, particularly in the Midwest and states like Texas, Iowa, and Kansas. By investing in these hospitals, the RHTP aims to prevent closures, preserve essential services like emergency and maternity care, and improve health outcomes in rural America.
Contact AvaSure to discuss how you can use RHTP funding for virtual care.
How can telehealth and virtual care benefit rural hospitals?
RHTP applications from numerous states have revealed a priority among rural hospitals: the use of telehealth and virtual care to help extend and improve care where things like specialty care are often unavailable.
By integrating telehealth, rural facilities can bridge the “specialty gap,” allowing local doctors to consult with world-class neurologists or cardiologists in real-time without transferring the patient. This “keep it local” approach not only improves patient outcomes during emergencies but also stabilizes the hospital’s finances by retaining admissions and reducing the reliance on expensive traveling staff. In addition, by leveraging AI and virtual care, rural hospitals can expand local access and boost financial sustainability while delivering higher-quality care. These innovations do more than just improve patient outcomes and ROI; they actively reduce safety risks like falls, alleviate staff burnout, and foster collaborative models of care. See how Hackensack Meridian Health improved nurse satisfaction and patient outcomes through virtual nursing.
How do states plan to use their funding for the Rural Health Transformation Program (RHTP)?
States submitted plans in December 2025 that had to meet specific criteria defined by CMS. Funding for these plans was released in January 2026. The plans had to address how hospitals will:
Prioritize the use of new and emerging technologies including AI to improve rural health outcomes
Improve access to care locally
Enhance quality metrics for rural patients
Foster partnerships (e.g. small hospitals collaborating with larger systems) and ensure financial stability of rural providers
Tackle causes of rural hospital closure
How can hospitals leverage RHTP funding?
1. Engage State RHTP Leadership
Coordinate with your state health department or Medicaid agency to include virtual care in your Rural Health Transformation Plan. Highlight its impact on workforce resilience and patient safety.
To strengthen your case, align the stated goals to the RHTP program and track them. The outcomes that AvaSure has benchmarked with partner hospitals with virtual care programs are:
72% improvement in 1:1 sitter usage
11.6% improvement in length of stay
26% improvement in RN overtime
30-50% improvement in falls
4. Build a Sustainable Model
Reinvest efficiency savings and improved performance outcomes to sustain virtual nursing operations post-RHTP funding.
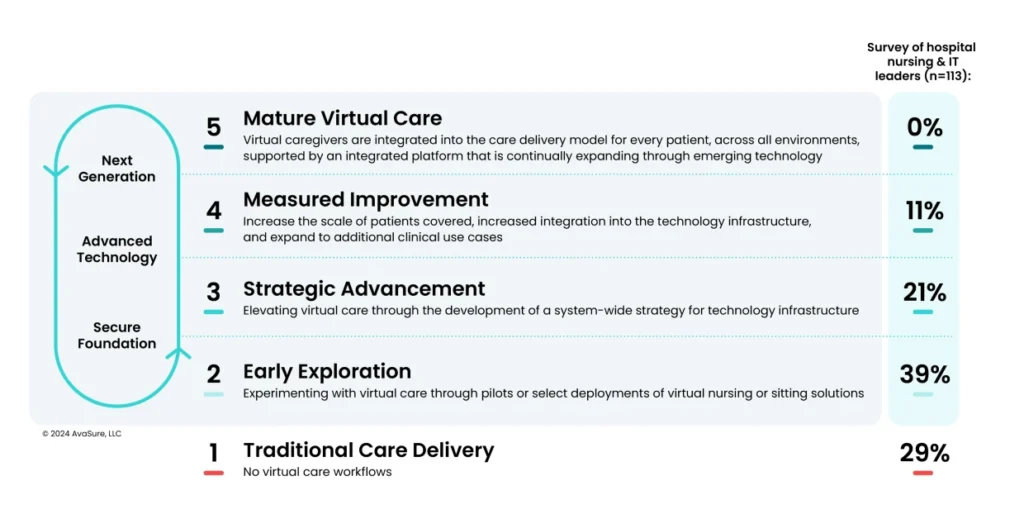
AvaSure’s maturity model provides a strategic roadmap for health systems to transition from initial pilots to a fully integrated virtual care delivery system. It serves as a vital framework for leaders to benchmark their current capabilities and identify the specific infrastructure and workflow milestones required to reinvest efficiency savings and sustain high-performance virtual nursing long after the conclusion of RHTP funding.
How AvaSure Aligns with the Rural Health Transformation Program
AvaSure, the industry leader in virtual nursing and continuous patient monitoring, helps hospitals extend nursing capacity, reduce falls and sitter costs, and enhance care quality through a proven operational model. AvaSure’s virtual care platform is fully aligned with RHTP’s focus on technology-enabled workforce transformation.
RHTP Funding Categories Supported by AvaSure:
Workforce development and modernization
Technology-enabled patient care and safety
Training and technical assistance
Quality and efficiency improvement initiatives
The Rural Health Transformation Program prioritizes initiatives that stabilize and modernize the healthcare workforce, improve patient safety, and enable sustainable operations in rural hospitals. AvaSure supports all three objectives by bringing virtual nursing and continuous observation into daily hospital operations:
Virtual Nursing: Augments bedside teams with remote nurses who handle admissions, discharges, and patient education to reduce admin burden.
Continuous Observation (TeleSitting): Centralized video observation reduces falls, elopements, and 1:1 sitter costs.
Specialty Consults: Consult with specialists in another location to expand care without having to move your patient.
This in turn leads to benefits such as:
Workforce Flexibility: Reduces overtime, improves staff retention, and increases productivity.
Patient Safety: Delivers continuous monitoring and rapid response support.
Ultimately, access to care and physician specialists remains one of the most pressing challenges for rural hospitals, leading many to prioritize specialty health and telehealth consults in their strategic applications. To effectively remedy these gaps, it is essential to select a virtual care platform that leverages the specific partnerships necessary to bridge the distance between patients and specialized expertise.
How Can AvaSure Help?
AvaSure’s partnership with Equum Medical, a telehealth-enabled clinical workforce organization, will provide rural hospitals with easy access to virtual specialty consults. The company’s broad portfolio of services addresses the driving challenges of Access and Capacity for health systems, including multi-specialty telemedicine, critical care, virtual nursing, virtual sitter monitoring, and telemetry. Solutions include:
Tele-ICU and critical care support, including surge capacity and after-hours coverage
Virtual hospitalist support for nights, weekends, and hard-to-staff locations
Care coordination that helps reduce avoidable transfers, keep patients local, and support patient flow with integrated virtual nursing capabilities across care venues
These solutions strengthen financial sustainability while offering scalable, broadband-friendly technology specifically designed for the unique constraints of rural settings. Unlike typical telehealth partnerships that add separate point solutions, the integrated model runs on a single platform that many hospitals already use for virtual nursing and patient observation, paired with Equum’s physician and clinical programs.
Your RHTP Virtual Care Strategy
AvaSure equips rural hospitals with innovative virtual care and AI-powered solutions that expand local access, enhance care quality, and strengthen financial sustainability. By reducing adverse events like patient falls, easing workforce burdens, and fostering collaborative models of care, AvaSure helps rural providers meet and exceed the goals of the Rural Hospital Transformation Program.
Posted on February 18, 2026 by Maura Kretzer - Uncategorized
How Providence St. Peter Hospital and Providence Oregon Improved Caregiver Safety Through Remote Visual Monitoring
Overview
Workplace violence has become a critical challenge across health systems, affecting caregiver morale, patient safety, and the overall care environment. Providence St. Peter Hospital in Washington and the Providence Oregon region implemented a virtual care monitoring program using AvaSure technology to proactively reduce violent incidents and protect staff and patients. Their experiences demonstrate how virtual engagement, predictive monitoring, and strong interdepartmental collaboration can dramatically improve safety outcomes. [Eyes on Sa…Transcript | Word]
Challenge
Both regions were seeing increases in:
Physical and verbal aggression toward nurses and CNAs
Visitors introducing illicit substances or behaving violently
Patients harming themselves or attempting to harm caregivers
False allegations against staff, creating legal and safety risks
Traditional approaches—such as staff rounding and signage—offered awareness but not reliable prevention. Violent events were still leading to caregiver injuries and unsafe environments. [Eyes on Sa…Transcript | Word]
Solution: Remote Visual Monitoring (RVM) with AvaSure
Protecting staff during a bathroom attack, when techs saw nurses running out of the room and immediately called security. [Eyes on Sa…Transcript | Word]
These cases highlight how remote monitoring enables fast intervention, even when staff cannot directly see risk evolving.
Culture & Governance Enhancements
Both regions emphasized:
Violence Prevention Committees with nurses, security, and leaders to review events and coordinate improvements. [Eyes on Sa…Transcript | Word]
Regular communication via huddles, newsletters, SharePoint, and site visits to build trust between bedside staff and monitoring techs. [Eyes on Sa…Transcript | Word]
Empower virtual safety attendants: instruct them to call security even if bedside staff says, “We’re okay.” Better to over-respond than underrespond. [Eyes on Sa…Transcript | Word]
Providence St. Peter Hospital and Providence Oregon successfully transformed their approach to workplace violence by integrating virtual care monitoring into daily operations. Their experiences show that proactive surveillance, empowered staff, and clear escalation pathways can significantly reduce risk and create safer environments for caregivers and patients alike.
This case study demonstrates how modern virtual care infrastructure—used thoughtfully—serves as both a protective shield and a tool for continuous care improvement.
Hospitals are under pressure to reduce preventable harm from falls, elopement, and other adverse events while maintaining a sustainable workload for clinicians. Camera-based monitoring and virtual sitting programs such as AvaSure’s Continuous Observation platform have already demonstrated that continuous observation can reduce falls and injuries, but human-only monitoring does not scale indefinitely. Many organizations are now exploring Artificial Intelligence to extend the reach of their teams, and to detect risk earlier than a human observer might be able to do consistently.
At AvaSure, we view Artificial Intelligence as an extension of the virtual care platform that more than 1,200 hospitals already use for continuous observation, virtual nursing, and specialty consults. Our goal is not to replace human judgement. Instead, we want to build behavior-aware monitoring that can recognize patterns associated with risk, surface those patterns to caregivers in time to intervene, and do so in a way that is technically sound, clinically grounded, and respectful of patient privacy.
This blog describes the design principles behind our Falls and Elopement Artificial Intelligence system. AvaSure leverages Computer Vision, a subset of Artificial Intelligence, to detect high-risk scenarios before an adverse event occurs. Our Computer Vision models perceive the hospital room environment by learning what situations are unsafe for patients. This allows us to demonstrate the clinical performance of our models made possible by our onboarding process for new hospitals. Built on Oracle Cloud Infrastructure (OCI), this cloud-based system provides a scalable foundation that extends beyond fall and elopement prevention into broader ambient AI applications.
What are the Challenges of Computer Vision Models for Falls and Elopement?
Falls and elopements rarely occur as single, isolated moments. They emerge over a sequence of behaviors. A patient may shift position in bed, sit upright, move to the edge of the bed, stand, and then begin to move away. However, there are challenges to building Computer Vision models that understand such behavior. Staff and visitors come and go, sometimes obstructing the view of the camera. Lighting changes over the course of the day and night, including the use of infrared lighting in low light situations. All these challenges are part of the design space, and a monitoring system that considers a single video frame at a time without regard to such confounding elements can miss much of this context.
An important way to adapt to these challenges is to select the right type of camera device. Choosing the right device for AI for patient safety also impacts how the system perceives the hospital room environment. AvaSure offers a variety of camera devices including Guardian Dual Flex, Guardian Mobile Devices, and Guardian Ceiling Devices. Guardian Dual Flex devices provide a fixed camera dedicated to Artificial Intelligence monitoring. Mobile units introduce variation in pan, tilt, zoom, and location within the room – each of which varies in layout across and within different hospital systems. Guardian Ceiling devices provide a different perspective compared to Dual Flex and Mobile devices.
AvaSure’s Computer Vision system and onboarding processes are built to adapt rather than assuming a single, fixed installation environment. Our current models for Falls and Elopement focus on understanding posture and presence over time while accommodating variations in lighting and environment. The system distinguishes the posture of the patient from lying in bed, sitting on the side of the bed, or standing. These states are evaluated over short time windows and combined with rules that relate them to risk. For example, a transition from lying to sitting on the side of the bed may be treated as an early warning, whereas a transition to standing unassisted may prompt a higher-severity alert.
How Does Falls and Elopement AI Perceive the Patient Room?
The Falls and Elopement models employ a three-layer approach to perceive conditions within the hospital room.
Lowest Layer: Detect whether there are people in the frame and estimate how many.
Middle Layer: When there is a single person in view, form an understanding of posture and location relative to the bed and other furniture.
Top Layer: Combine these posture estimates over time and apply rules that map temporal patterns to alerts.
This layered approach is intentional. Computer vision research has shown that models built only around pose estimation can struggle with common conditions in clinical rooms, such as occlusions from blankets and equipment, low light, and cluttered backgrounds. By combining person detection with semantic posture classification and temporal reasoning, we maintain flexibility in camera hardware while capturing clinically meaningful patterns in the room.
The temporal aspect is central to how the system works. Rather than categorizing each frame in isolation, the models consider short windows of behavior and pay attention to transitions. A single frame showing a patient near the edge of the bed may not be sufficient to decide whether they are attempting to stand or simply shifting position. A sequence of frames that show a consistent movement from reclined to upright to standing is more informative. Alerts are based on this kind of sequence-aware understanding rather than a momentary snapshot.
AvaSure designs for known sources of variability. Mobile cameras introduce changes in viewpoint and zoom as they are repositioned. Different rooms may be arranged in mirror images, with beds and bathrooms on opposite sides. Lighting can range from bright daytime scenes to low-light conditions at night. During model development and onboarding, we deliberately include these variations so that the system can learn to interpret similar behaviors across a range of visual conditions.
How does AI for Patient Safety Learn Real-World Clinical Complexity?
Computer Vision models learn by being fed many examples of different situations. For example, these could be labeled as “a patient lying in bed” or “a patient standing near the side of the bed”. The learning (or training) process then iteratively adjusts the model parameters based on how well the model at that iteration correctly predicts the situation associated with a given example. This process repeats until the model performs well enough. There are several methods for capturing data for training, including having actors stage scenes and having computers generate synthetic scenes by rendering life-like situations.
However, models trained only on staged scenes and synthetic data tend to perform best on those same controlled scenarios. Real hospital rooms are more complex. Patients vary widely in demographic, mobility, and behavior. Equipment is added and removed. Staff and visitors move through the field of view in unpredictable ways. To build models of AI for patient safety that can handle this complexity, we need to learn from images that reflect it. At the same time, patient identity and privacy must be preserved.
AvaSure maintains a patent-pending patient anonymization system that allows us to incorporate real-world imagery into training and evaluation without retaining identifiable visual information. The system applies transformations that remove or obscure personally identifiable features and present them to a human reviewer. The reviewer confirms that anonymization is complete and assigns labels describing the posture and relevant contextual details. Only after this confirmation do the frames enter curated data sets used for training and for measuring performance in production.
The system captures frames concentrated around ambiguous or clinically relevant situations rather than random samples of uneventful periods. This makes them particularly useful for improving model performance for video cases where decisions are hardest.
Precision vs Recall: Which Metrics Matter Most for Clinical Success?
When evaluating models in safety-critical domains, accuracy alone is not sufficient. Falls and elopements are relatively rare events compared with the number of hours of observation across a hospital. A system can achieve high overall accuracy by correctly labelling long periods of low-risk behavior yet still miss important events or generate more alerts than staff can reasonably handle.
For this reason, AvaSure frames performance in terms that reflect the realities of clinical operations. Precision captures how often an alert corresponds to a meaningful event. Recall captures how often the system detects an event when it occurs. The F1 score combines the two into a single measure that balances false positives and missed detections. These metrics tell us how often the system asks for attention when it is truly warranted and how often it remains silent when it should speak up.
In practice, different hospitals and units may prefer different trade-offs. A neurosurgical ward may choose to tolerate more alerts in exchange for fewer missed events, whereas a lower-acuity unit may prioritize reducing unnecessary interruptions. Our models can operate at different points along the precision-recall curve, and part of the onboarding process is to discuss and tune that operating point together with clinical and operational leaders.
Beyond the initial deployment, AvaSure treats performance as something that must be monitored and maintained. As room layouts, staffing patterns, and patient populations change, the distribution of behaviors the system sees will change as well. By sampling outputs in the field for new models running side by side with existing models, we can compare new model versions against established baselines and roll back changes that do not meet defined criteria.
Deployment Without Disruption: What is the Process for Onboarding New Hospitals with AI for Patient Safety?
For hospitals, the most important questions are how the system will behave in their specific environment and how disruptive deployment will be. AvaSure’s onboarding process is designed to answer those questions incrementally and transparently.
The work begins with understanding room configurations, typical camera locations, and the kinds of patients and use cases each unit expects to monitor. This can include having AvaSure team members stage representative scenarios in sample rooms, capturing video that reflects local layouts, lighting, and camera angles. This staged data helps verify that the baseline model behaves as expected before any live patient feeds are involved.
As cameras are connected, we run the models in background mode. The system processes live video, but alerts are not yet sent to staff. During this period, we collect anonymized frames of interest and review the patterns of potential alerts. This is also when we fine-tune the operating point where we can adjust the precision vs recall for the unit’s needs.
Once the hospital is comfortable with the system’s behavior, alerts are enabled for virtual safety attendants. The user interface will increasingly support structured feedback so that attendants can indicate whether an alert was helpful, spurious, or associated with an event the system should have recognized. These feedback signals, together with anonymized frames, feed back into our data and model improvement process. By gathering room dimensions, lighting, and arrangement details, we are able to use rendered scenes that are specific to each environment, streamlining the creation of training examples for new hospitals.
How to Extend Beyond AI for Patient Safety Monitoring
Falls and elopements are a natural starting point for behavior-aware monitoring because they are common, clinically important, and directly connected to existing continuous observation workflows. However, the same sensing and inference capabilities can support a broader set of safety and quality use cases over time.
AvaSure’s AI Augmented Monitoring strategy anticipates an expansion from Falls and Elopement into additional use cases such as hospital-acquired pressure injury prevention, infection-related behaviors, and staff duress. Environmental sensing capabilities, including detection of meal tray delivery and removal or patterns of in-bed movement, can contribute to these use cases by providing objective, continuous signals about patient status and care processes. Each new application will require its own feasibility studies, data collection plans, and validation steps, but they build on the same underlying platform and design approach.
Each of these additional use cases requires enhancements to the Computer Vision models to have them comprehend a wider variety of situations. Such enhancements can require additional or more complex models requiring additional computing power. AvaSure leverages OCI’s AI infrastructure offerings to bring to bear considerable GPU-powered computing to support an expanding range of use cases.
How do we integrate security and compliance into the design of healthcare AI models?
Security for us is not a separate track from Artificial Intelligence; it is part of the design of the platform and the models from the beginning. AvaSure’s virtual care systems already operate in environments where SOC 2 and HIPAA expectations are the baseline, not an add-on, and the same standard applies to AI Augmented Monitoring. Every new service that touches patient data, from model pipelines to anonymization computing, is expected to pass formal design review, threat modelling, and, where appropriate, penetration testing before it is considered ready for production.
At the infrastructure level, our cloud strategy is built on a scalable, multi-tenant architecture designed to keep different users and services securely separated. Robust identity and access management ensures that only authorized components can communicate or access sensitive data, and every service operates with the minimum permissions required. Data moving through the system is protected by encryption, as is data stored in managed services. Comprehensive audit logging is a core part of our approach, recording authentication and authorization events, configuration updates, model changes, and administrative actions so that security and compliance teams can thoroughly review activity if needed.
For AI specifically, the same security-by-design approach applies. Security specialists review designs for new AI use cases during ideation rather than waiting for prototypes. The review looks at how video streams enter the system, where inference is performed, what outputs persisted, and how PHI is handled or removed. This helps ensure that the introduction of GPU-backed inference or new data flows does not inadvertently expand the attack surface or weaken isolation guarantees.
The anonymization pipeline is an example of security and privacy concerns shaping the technical design. Rather than storing raw patient video, the system extracts short windows around events of interest and routes them to a separate anonymization service. That service applies privacy preserving transforms and requires human confirmation that identifiable information has been removed before frames can be used for training or evaluation. All of this traffic is encrypted in transit; anonymized images are encrypted at rest and stored with restricted access. This architecture allows the models to benefit from realistic data while maintaining clear boundaries around PHI.
In practice, ensuring security involves closely connecting monitoring activities with incident response protocols. A comprehensive strategy includes full observability across systems and processes, using tools like metrics, alerts, dashboards, and health checks to quickly detect and respond to any unusual activity. The same mechanisms that support autoscaling and automated rollback for availability also support security; if a change in configuration or dependency were to introduce unexpected behavior, operators can detect it quickly and revert. Regular risk assessments, combined with continuous integration and deployment practices, are intended to keep the platform aligned with evolving threats and regulatory expectations rather than treating compliance as a static checklist.
From the hospital’s perspective, the outcome of this approach should be straightforward: AI features sit inside a platform that is already held to enterprise security and compliance standards, and any new capability is expected to meet those standards before it is offered in production. The same controls that protect virtual care today – access control, encryption, audit logging, and formal review – apply equally to behavior-aware monitoring and future AI use cases.
How Does AvaSure Scale AI for Patient Safety in Modern Health Systems?
Building AI for patient safety is not simply a matter of choosing a model architecture or training on a large data set. It is a system-level effort that spans model design, data collection, anonymization, infrastructure, onboarding, monitoring, security, and governance. Each part influences how the technology behaves in practice and how much clinicians and patients can rely on it.
For AvaSure, the core elements of that system are clear. We focus on understanding behavior in context rather than isolated frames. We adopt a stepwise development approach that involves staged experiments, demonstrations, and validation in real clinical settings. We learn from real rooms through an anonymization data collection system that protects identity while concentrating on data where it matters most. We operate on a cloud platform designed for reliability, scalability, and security. Lastly, we treat hospitals as partners in an ongoing improvement process rather than one-time installations.
AvaSure is building AI for patient safety into the virtual care platform that customers already use for continuous observation and virtual nursing. Future blogs will explore specific components in more depth, including anonymization and data curation, our hybrid edge–cloud roadmap, and the evolution from single-use models to a suite of AI augmented monitoring applications. For now, our aim is to make the underlying approach visible so that hospital leaders and clinicians can make informed decisions about how AI fits into their own patient safety strategies.
While most IT and clinical leaders believe that inpatient acute virtual care will play an increasingly significant role in care delivery, the reality is that it is still in the early stages of adoption. Survey data reveals a surprising gap: 29% of organizations have no virtual care programs, even as hospital leaders rank it as a top priority.
To help organizations bridge this gap, the 5-stage Inpatient Virtual Care Maturity Model offers a comprehensive blueprint for care model redesign, empowering leaders to drive change management and implement manageable, outcome-focused strategies.
What stage is your organization? Download the report to learn:
Where hospitals currently stand in virtual care maturity
How virtual care is reducing the burden on bedside staff
The key metrics hospitals use to measure virtual care program success
Falls remain a persistent and costly issue among hospitalized veterans, who are at a higher risk due to more prevalent chronic conditions. In response, the Veterans Health Administration introduced the SAFE STEPS for Veterans Act in 2024, creating an Office of Falls Prevention. Staffing shortages, particularly among Patient Care Technicians and Certified Nursing Assistants have exacerbated patient safety concerns, with patient falls rising 253% from 2020 to 2022.
To reduce the need for 1:1 sitters and improve safety, AvaSure’s AI-powered virtual care platform enables hospitals to remotely monitor high-risk patients and prevent falls and other adverses events.
Download the guide to learn:
How to reduce falls by nearly 20%
Ways to improve staff efficiency & satisfaction
The top 4 adverse events prevented in VA hospitals
Passionate and dedicated, the virtual sitters at VA North Texas Health Care System transcend their virtual presence, forming genuine bonds with the veterans they care for. Nurse manager Tiffany Villamin shared a poignant anecdote at the 2023 ANCC National Magnet Conference®, illustrating the profound impact of these virtual heroes. When an impending ice storm threatened, these compassionate individuals proactively offered support, ready with sleeping bags in hand, demonstrating their unwavering commitment to the veterans and bedside staff.
A Success Story in Virtual Sitting Implementation
VA North Texas Health Care System, comprising 13 facilities and over 700 beds, stands as a beacon of success in virtual sitting adoption. Since embracing this technology, the health system achieved a remarkable 20% reduction in inpatient fall rates and slashed hourly patient sitting costs by nearly 90%.
Addressing Patient Safety Challenges
Facing labor shortages and escalating costs, VA North Texas prioritized patient safety and fall prevention. Recognizing the superiority of virtual sitting over traditional one-to-one sitting, the health system implemented a program leveraging 2-way video and audio capabilities. This centralized monitoring hub, staffed by virtual safety attendants, oversees up to 48 cameras, effectively reducing patient falls.
Results: Lower Costs, Improved Patient Safety
The impact of virtual sitting at VA North Texas is profound. By freeing frontline staff for direct patient care and decreasing 1:1 sitter usage, the program saved an average of 83 full-time equivalents per month, translating to an annual savings of $3.4 million. The efficiency gains are substantial, with costs per virtual sitting hour reduced to $3.05 compared to $26 for one-to-one sitters. Fall rates plummeted by nearly 20%, well below national averages.
Expanding Impact and Enhancing Care
Looking ahead, VA North Texas plans to extend the program to the Emergency Department and mental health department, further enhancing patient safety and care delivery.
Conclusion
Virtual sitting represents a transformative approach to patient care, yielding cost savings and improved outcomes. VA North Texas Health Care System exemplifies the potential of this technology to revolutionize healthcare delivery, ensuring better patient outcomes and optimized resource utilization.
Awards program recognizes individuals and organizations for advancing patient and staff safety
BELMONT, Mich., [May 15, 2024] — AvaSure, a market leader in acute virtual sitting and virtual nursing, proudly unveils five recipients of the 2023 AvaPrize awards.
AvaSure’s virtual care awards program, AvaPrize, recognizes individuals and organizations whose unwavering dedication has not only enhanced patient safety but has also revolutionized the nursing experience and ushered in new standards of care efficiency.
“At AvaSure, we are on a mission to redefine healthcare delivery by harnessing the power of technology,” said Adam McMullin, CEO, AvaSure. “We stand alongside the nation’s leading health systems in championing transformative care models that prioritize patient safety, empower nursing teams, and drive tangible improvements in outcomes. It is with great pride that we pay homage to these exceptional individuals and organizations for their tireless commitment to leveraging intelligent virtual care to shape a brighter future for healthcare.”
2023 AvaPrize winners
The Hub & Spoke Award recognizes the organization with the most efficient use of the AvaSure platform by multi-site organizations using a single remote central observation center. The award went to the University of California San Diego Health – Hillcrest, which has significantly improved patient safety while reducing the use of one-to-one sitters through its virtual sitting program. The program has enabled the health system to sustain an ongoing annual sitter avoidance of 20 patients per day, or the equivalent 84.0 full-time equivalents (FTEs).
The SafetyNet Award honors the organization that demonstrates the most complete AvaSure virtual care program. In 2023, that was PeaceHealth St. Joseph Medical Center, which has used the AvaSure platform to improve care for patients with dementia and those at risk of self-harm. Across eight of its facilities, the health system monitored 16,463 patients for 1,317,917 hours in 2023, preventing a staggering 121,249 adverse events.
The Path to Zero Award recognizes an organization focused on patient safety, specifically with reducing fall rates with the AvaSure platform. In 2023, the award went to Centra Health, whose team leveraged the real-time analytics and quality dashboards to help progress and track the reduction of falls.
The Super Star Virtual Safety Attendant Award recognizes individuals who consistently exceed expectations in ensuring the successful utilization of the AvaSure platform. The award went to Dorcus Poku of VHC Health, a virtual sitting technician who has consistently demonstrated an unwavering commitment to her role.Beyond ensuring the effective use of the AvaSure platform, Poku ensures that compassionate patient care is not lost in virtual settings. Her ability to establish meaningful connections with patients under her care, as well as with the clinical staff, sets her apart as a true asset to the healthcare team.
The VA Award honors the remarkable advancements in virtual care achieved by VA Hospitals. In 2023, the winner was W.G. Bill Hefner Salisbury Department of Veterans Affairs Medical Center, emblematic of its pursuit of innovation and improvement to provide the best care to our Veterans. The team actively seeks and implements best practices, fostering a culture of continuous improvement and unwavering commitment to delivering exceptional care. Furthermore, their collaborative spirit extends beyond their institution as they generously share their insights and experiences with other VA facilities, progressing and elevating standards across the VA health system.
The AvaPrize awards have been personally delivered, allowing the AvaSure team to express heartfelt gratitude to each recipient for their remarkable dedication to implementing technology-driven solutions in the pursuit of unparalleled patient care.
To learn more about the 2023 AvaPrize winners, click here. 2024 submissions are now open.
About AvaSure AvaSure® is an intelligent virtual care platform that healthcare providers use to engage with patients, optimize staffing, and seamlessly blend remote and in-person care at scale. The platform deploys AI-powered virtual sitting and virtual nursing solutions, meets the highest enterprise IT standards, and drives measurable outcomes with support from care experts. AvaSure consistently delivers a 6x ROI and has been recognized by KLAS Research as the #1 solution for reducing the cost of care. With a team of 15% nurses, AvaSure is a trusted partner of 1,100+ hospitals with experience in over 5,000 deployments.
Media contact: Marcia G. Rhodes / mrhodes@acmarketingpr.com