Use Cases, Benefits, and Considerations for Hospitals
What is TeleSitter?
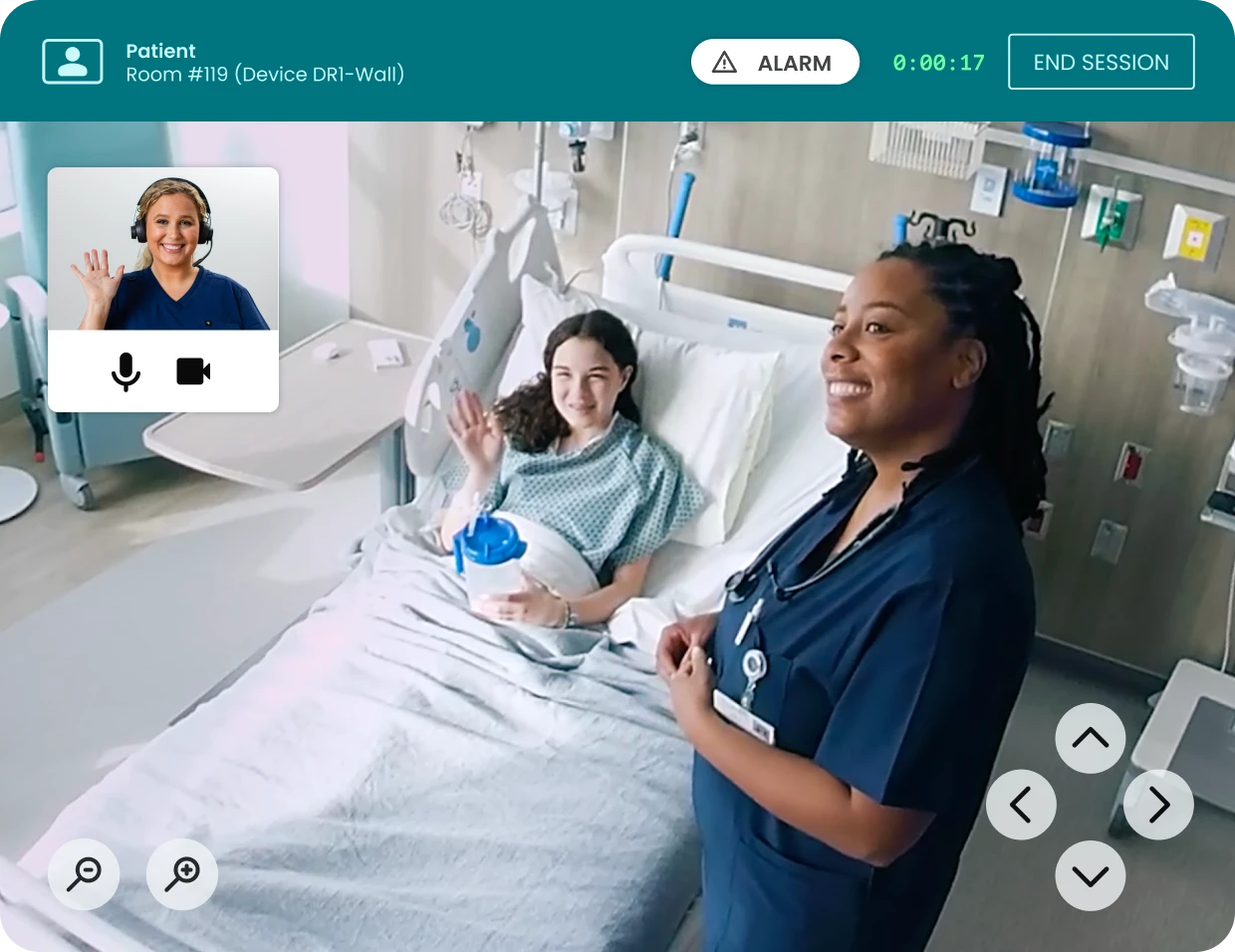
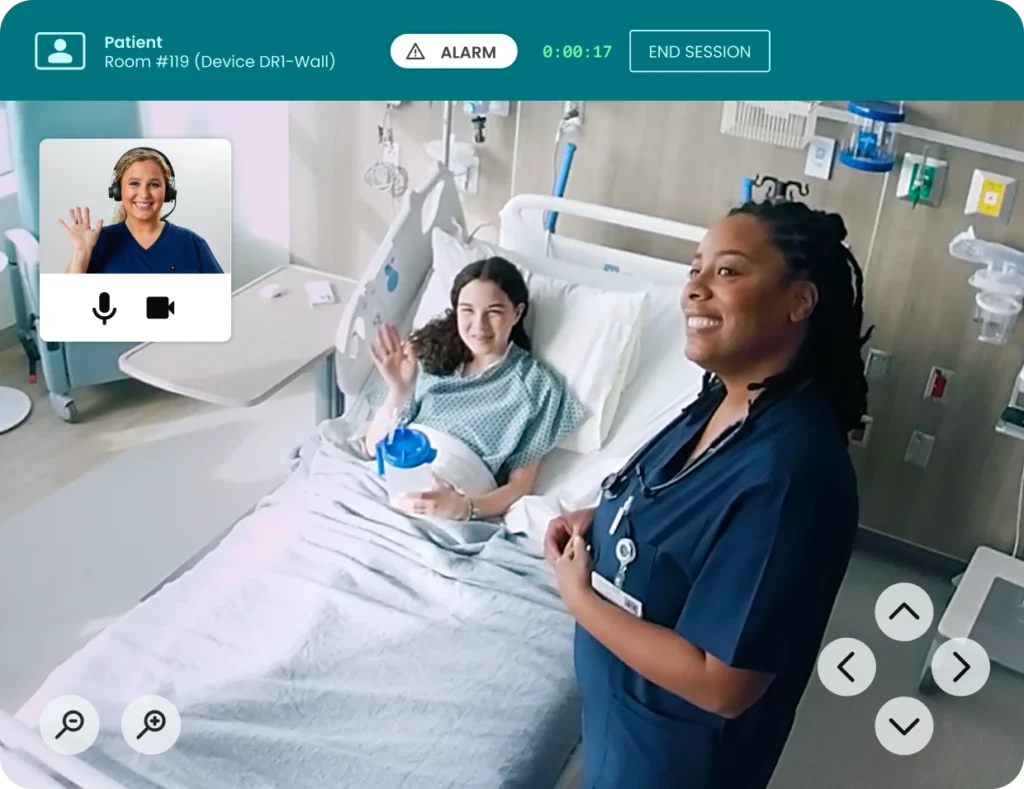
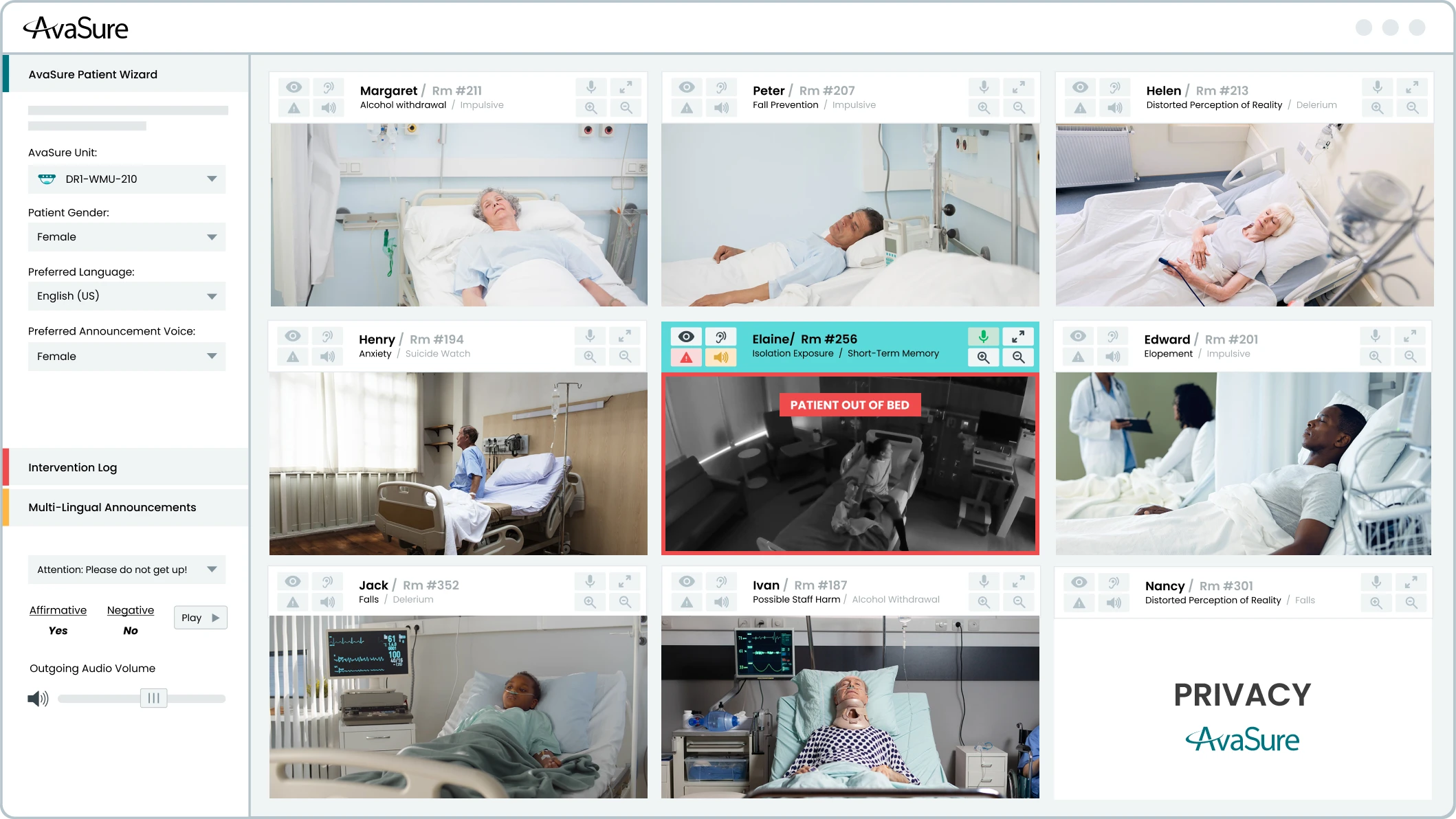
TeleSitter is a continuous remote patient monitoring platform used in hospitals that allows a single trained virtual safety attendant (VSA) to monitor multiple at-risk patients simultaneously. The VSA uses the solution to prevent patient falls and elopement, workplace violence, and behavioral health risks.
AvaSure invented the TeleSitter® solution in 2008, creating a category-defining remote patient observation technology designed to help hospitals reduce the cost and dependency of one-to-one bedside sitters while maintaining patient safety. The TeleSitter solution delivers a 6x ROI, reduces adverse events by over 50%, reduces reliance on 1:1 sitters by up to 90%, and brings nursing staff back to the bedside.
What does TeleSitter do?
TeleSitter enables a single virtual safety attendant to monitor multiple at-risk patients simultaneously on one screen to prevent falls, elopement, workplace violence, and behavioral health risks.
Common use cases for virtual sitting:
Fall Prevention
One of the most common use cases for TeleSitter is fall prevention. Virtual Safety Attendants use the TeleSitter application to monitor patients at risk of falls. If they see a patient getting out of bed or not listening to instructions, they can send automated voice commands, speak directly to the patient, or activate the stat alarm — a loud, audible alarm in the patient’s room — to alert bedside care team members that a patient needs immediate assistance. This alarm can be routed through nurse call, mobile devices, or dome light systems for immediate action. Hospitals using TeleSitter have documented fall rate reductions exceeding 50%, and one health system saved $3.2 million from sitter cost reductions and avoided fall-related costs, while another saved $1.5M in just one year. However, while keeping patients safe from falls is where this technology started, it’s only the beginning of what it can do.
Elopement Prevention
Elopement prevention is another one of the most common use cases of TeleSitter. Patients who are disoriented, cognitively impaired, or in a behavioral health crisis can move quickly, and by the time a bedside nurse notices something is wrong, precious time has already been lost. Virtual Safety Attendants and AI monitoring are trained to recognize the early behavioral cues that precede an elopement attempt — restlessness, repositioning, reaching for side rails — and intervene verbally before a patient ever gets to the door.
Workplace Violence Prevention
TeleSitter can also be used to prevent workplace violence. Healthcare workers face a disproportionately high risk of violence compared to workers in other industries, and placing a 1:1 sitter physically in the room of an agitated patient doesn’t always make that situation safer. Virtual monitoring allows staff to observe, de-escalate, and call for backup from a position that keeps everyone protected. For behavioral health patients more broadly, the ability to maintain a constant, calm, remote presence — one that can redirect without escalating — has proven to be a genuinely different kind of intervention than what a physical sitter can offer.
Low-to-Moderate Suicide Risk Monitoring
Suicide risk monitoring for patients assessed at low-to-moderate suicide risk is another use case for TeleSitter that has grown substantially and carries meaningful clinical backing. The Joint Commission has formally recognized video monitoring as an acceptable intervention for this patient group, which has given hospitals the confidence to deploy it more broadly across medical and emergency department settings. Research led by David Kroll, MD, of Brigham & Women’s Hospital in Boston, has shown that having a nursing assistant sitting in the room of a suicidal ideation patient is unproven in preventing self-harm. By contrast, use of the TeleSitter solution (now Continuous Observation) on suicide risk patients resulted in zero adverse events (Kroll, 2019). This initial study laid the foundation for The Joint Commission to deem virtual sitting an acceptable intervention for low and moderately suicidal patients.
Pediatric Patient Monitoring
TeleSitter can be used for pediatric patient monitoring through multiple use cases. Pediatric care presents its own unique set of scenarios — from adolescents hospitalized for eating disorders, where constant supervision during meals and bathroom visits is clinically necessary but enormously staff-intensive, to infants at risk of falls when exhausted parents doze off while holding them, to children with autism or developmental disabilities who require consistent, attentive oversight without the potential agitation that a stranger in the room can sometimes cause. In each of these cases, virtual sitting offers a way to maintain the standard of care without the staffing burden that would otherwise make it unsustainable.
Whether the goal is protecting a vulnerable patient, de-escalating a difficult situation, or giving an overstretched nursing team a little more capacity, virtual sitting has proven it belongs at the center of a modern patient safety strategy.
Benefits and limitations of TeleSitter
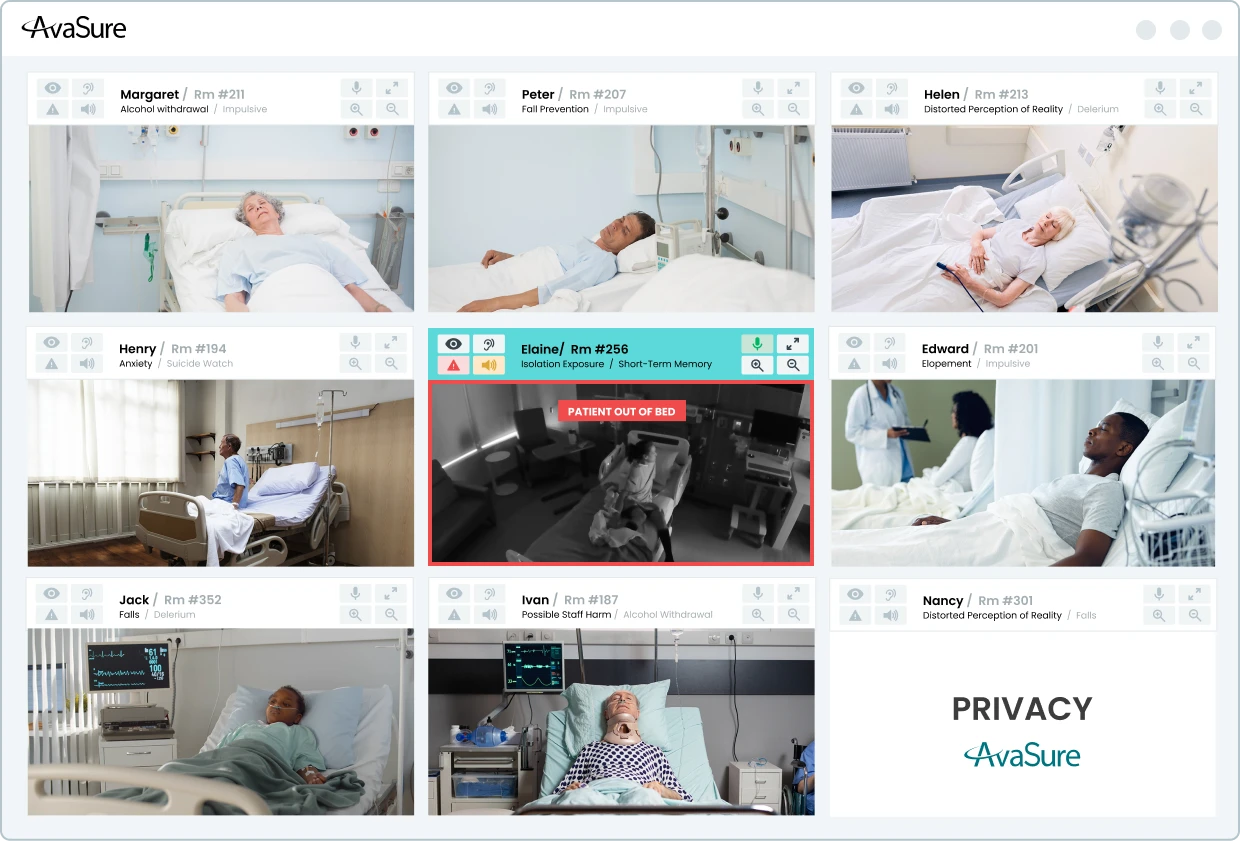
The benefits of virtual sitting are real and well-documented. The most straightforward case for virtual sitting is economic: replacing 1:1 bedside sitters with a model where a single Virtual Safety Attendant monitors up to 36 patients simultaneously dramatically changes the labor math. Decades of peer-reviewed research have established that virtual monitoring is not merely equivalent to in-person sitting — in several key areas, it has proven superior. For fall prevention, for suicide risk monitoring, and for workplace violence prevention, studies consistently show that the virtual model performs as well or better than traditional 1:1 observation, while also reducing the emotional and physical burden on nursing teams (The Evidence-Based Case for a Virtual Care Solution). Research published in the Western Journal of Nursing Research found that virtual sitting actively reduces nurse burnout, with bedside staff viewing virtual monitoring as a resource that supports them rather than adding to their workload. That’s a benefit that extends well beyond the patients being monitored.
One of the limitations of TeleSitter on its own is that it is inherently reactive and scope-limited. While TeleSitter focuses on surveillance and verbal intervention, it does little to address the broader staffing crisis, documentation burden, or clinical complexity driving nurse burnout and attrition. With burnout affecting 56% of the nursing workforce, health systems need more than a safety tool — they need a new model of care delivery.
That evolution is Virtual Nursing, which extends the same trusted in-room device beyond observation to support admissions, discharges, medication reconciliation, patient and family education, rounding, specialty consults, and novice nurse mentorship — all without switching platforms or disrupting existing workflows. Rather than simply watching patients, Virtual Nurses now actively offload documentation burden, close the experience gap created by staffing shortages, and help systems achieve measurable clinical and financial ROI.
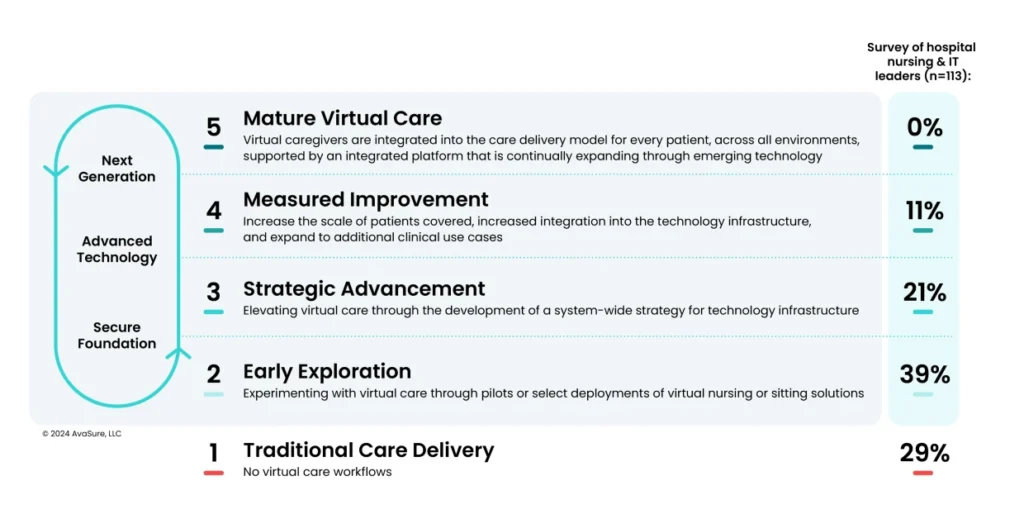
How TeleSitter solutions have evolved
Virtual care has expanded far beyond just virtual sitting. Thousands of health systems around the US have adopted full virtual care programs, where virtual sitting, virtual nursing, and AI workflows come together on one singular platform to streamline clinical workflows and enhance nurse and patient safety.
AvaSure has evolved far beyond its origins as the TeleSitter solution to become a comprehensive, AI-augmented Intelligent Virtual Care Platform trusted by more than 1,200 hospitals. The solution originally known as TeleSitter® is now called Continuous Observation, a name that better captures the platform’s modern capabilities: a single Virtual Safety Attendant monitoring up to 36 patients simultaneously, supported by ambient AI that detects potential adverse events before they occur. What began as a tool for remote patient safety monitoring has expanded into a unified platform supporting virtual sitting, virtual nursing, episodic consults, specialty care, and ambient AI — all running concurrently on a single in-room device. The Guardian DualFlex exemplifies this evolution: its dual-camera design pairs a 30x optical zoom PTZ camera for clinical workflows with a dedicated fixed wide-angle camera for AI, ensuring uninterrupted computer vision even during active patient consults. Five integrated microphones support ambient listening, voice command workflows, and future AI audio applications — all from one device mounted to the TV, wall, or ceiling. AvaSure’s open Partner API further extends the platform’s reach, enabling approved third-party ambient AI applications (such as Suki and Abridge for clinical documentation) to access device audio securely and write structured notes back to Epic1 flowsheets, without manual entry. AvaSure proudly holds Epic’s Inpatient Virtual Care Toolbox designation.
AvaSure continues to build the smart room of the future through purpose-built devices, an expanding AI platform developed, and deep EHR integration that makes virtual care a seamless, intelligent part of every patient interaction.
Contact AvaSure to learn more about how our virtual care platform can help keep both your patients and nurses safe.
Key Takeaways
- AvaSure invented the TeleSitter® solution in 2008, and it has since evolved to what is known today as Continuous Observation.
- The most common use cases for virtual sitting are fall prevention, elopement prevention, behavioral health monitoring, low to moderate suicide risk, workplace violence prevention, pediatric safety, isolation/infection prevention, pre-surgical monitoring and seizure monitoring.
- The TeleSitter® solution delivers a 6x ROI, reduces adverse events by over 50%, and reduces reliance on 1:1 bedside sitters by over 75% — returning nursing staff to the bedside and alleviating burnout.
- Hospitals using TeleSitter (now Continuous Observation) have documented fall rate reductions exceeding 50%, with one health system saving $3.2 million in sitter costs and avoided fall-related expenses, and another saving $1.5 million in a single year.
- Peer-reviewed research consistently shows that virtual monitoring performs as well as — or better than — traditional 1:1 observation for fall prevention, suicide risk monitoring, and workplace violence prevention, while also reducing emotional and physical burden on nursing teams.
- AvaSure has expanded well beyond its TeleSitter origins, evolving into a comprehensive Intelligent Virtual Care Platform deployed across more than 1,200 hospitals, supporting Continuous Observation, virtual nursing, episodic consults, specialty care, and ambient AI — all on a single platform.
Sources
1Epic is a registered trademark of Epic Systems Corporation.