The Rural Health Transformation Program (RHTP) provides $50B in CMS funding (2026–2030) to strengthen rural hospitals.
States submitted transformation plans prioritizing technology, workforce resilience, and AI.
Virtual nursing, TeleHealth, and tele-specialty consults directly align with RHTP goals.
Hospitals can use RHTP funds to reduce falls, overtime, sitter costs, and specialty care gaps.
Sustainable virtual care models reinvest efficiency savings beyond federal funding.
What is the Rural Health Transformation Program (RHTP)?
Rural and community hospitals face critical workforce shortages and financial distress, with nearly half operating at a loss as of 2023, according to an AHA analysis of RAND Hospital Cost data. To address these pressures and improve care quality, Congress established theRural Health Transformation Program (RHTP)under the 2025 One Big Beautiful Bill Act (OBBBA). This $50 billion Centers for Medicare & Medicaid Services (CMS) initiative (FY 2026–2030) provides $10 billion annually to strengthen rural healthcare and offset projected funding gaps.
How CMS Administers RHTP Funding
States are the direct recipients and had to submit a Rural Health Transformation Plan for CMS approval. Half of the funding is divided equally among participating states—guaranteeing at least $100 million per year for five years if all states join—while the other half is distributed via a CMS formula. This massive pool supports infrastructure, technology, and workforce improvements for nearly 1,800 rural hospitals and 60 million residents.
How Critical Access Hospitals (CAHs) Benefit from RHTP Funding
While all rural providers are eligible, the nation’s 1,350 Critical Access Hospitals (CAHs) stand to benefit most, particularly in the Midwest and states like Texas, Iowa, and Kansas. By investing in these hospitals, the RHTP aims to prevent closures, preserve essential services like emergency and maternity care, and improve health outcomes in rural America.
Contact AvaSure to discuss how you can use RHTP funding for virtual care.
How can telehealth and virtual care benefit rural hospitals?
RHTP applications from numerous states have revealed a priority among rural hospitals: the use of telehealth and virtual care to help extend and improve care where things like specialty care are often unavailable.
By integrating telehealth, rural facilities can bridge the “specialty gap,” allowing local doctors to consult with world-class neurologists or cardiologists in real-time without transferring the patient. This “keep it local” approach not only improves patient outcomes during emergencies but also stabilizes the hospital’s finances by retaining admissions and reducing the reliance on expensive traveling staff. In addition, by leveraging AI and virtual care, rural hospitals can expand local access and boost financial sustainability while delivering higher-quality care. These innovations do more than just improve patient outcomes and ROI; they actively reduce safety risks like falls, alleviate staff burnout, and foster collaborative models of care. See how Hackensack Meridian Health improved nurse satisfaction and patient outcomes through virtual nursing.
How do states plan to use their funding for the Rural Health Transformation Program (RHTP)?
States submitted plans in December 2025 that had to meet specific criteria defined by CMS. Funding for these plans was released in January 2026. The plans had to address how hospitals will:
Prioritize the use of new and emerging technologies including AI to improve rural health outcomes
Improve access to care locally
Enhance quality metrics for rural patients
Foster partnerships (e.g. small hospitals collaborating with larger systems) and ensure financial stability of rural providers
Tackle causes of rural hospital closure
How can hospitals leverage RHTP funding?
1. Engage State RHTP Leadership
Coordinate with your state health department or Medicaid agency to include virtual care in your Rural Health Transformation Plan. Highlight its impact on workforce resilience and patient safety.
To strengthen your case, align the stated goals to the RHTP program and track them. The outcomes that AvaSure has benchmarked with partner hospitals with virtual care programs are:
72% improvement in 1:1 sitter usage
11.6% improvement in length of stay
26% improvement in RN overtime
30-50% improvement in falls
4. Build a Sustainable Model
Reinvest efficiency savings and improved performance outcomes to sustain virtual nursing operations post-RHTP funding.
AvaSure’s maturity model provides a strategic roadmap for health systems to transition from initial pilots to a fully integrated virtual care delivery system. It serves as a vital framework for leaders to benchmark their current capabilities and identify the specific infrastructure and workflow milestones required to reinvest efficiency savings and sustain high-performance virtual nursing long after the conclusion of RHTP funding.
How AvaSure Aligns with the Rural Health Transformation Program
AvaSure, the industry leader in virtual nursing and continuous patient monitoring, helps hospitals extend nursing capacity, reduce falls and sitter costs, and enhance care quality through a proven operational model. AvaSure’s virtual care platform is fully aligned with RHTP’s focus on technology-enabled workforce transformation.
RHTP Funding Categories Supported by AvaSure:
Workforce development and modernization
Technology-enabled patient care and safety
Training and technical assistance
Quality and efficiency improvement initiatives
The Rural Health Transformation Program prioritizes initiatives that stabilize and modernize the healthcare workforce, improve patient safety, and enable sustainable operations in rural hospitals. AvaSure supports all three objectives by bringing virtual nursing and continuous observation into daily hospital operations:
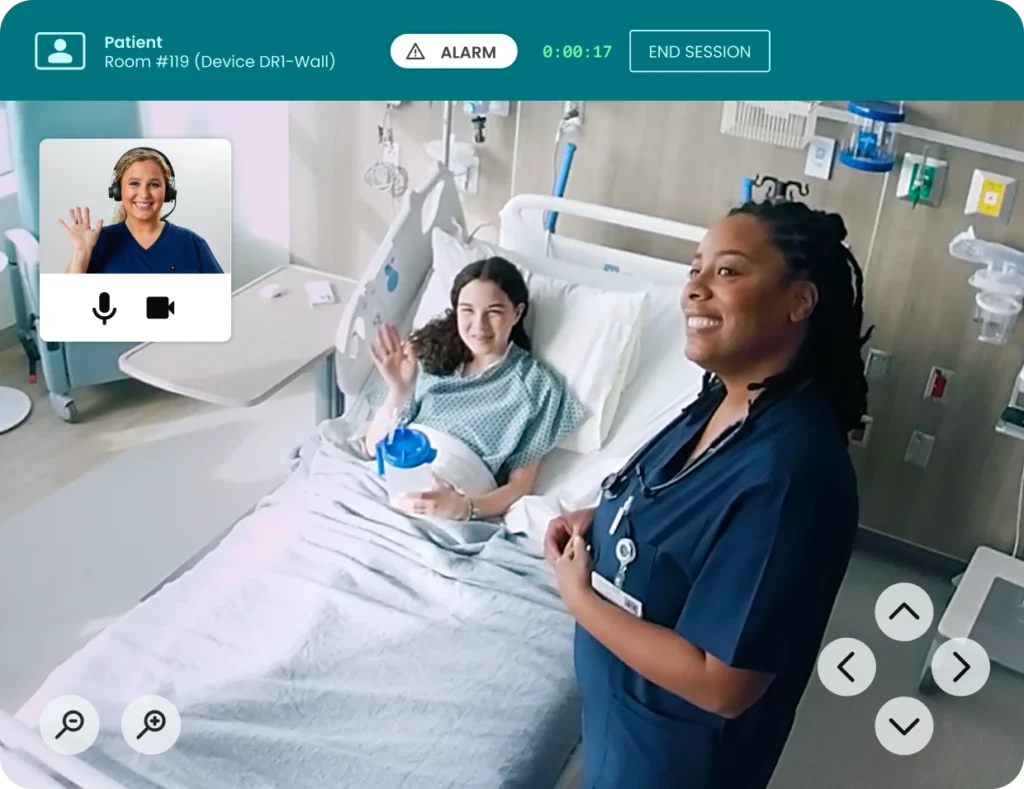
Virtual Nursing: Augments bedside teams with remote nurses who handle admissions, discharges, and patient education to reduce admin burden.
Continuous Observation (TeleSitting): Centralized video observation reduces falls, elopements, and 1:1 sitter costs.
Specialty Consults: Consult with specialists in another location to expand care without having to move your patient.
This in turn leads to benefits such as:
Workforce Flexibility: Reduces overtime, improves staff retention, and increases productivity.
Patient Safety: Delivers continuous monitoring and rapid response support.
Ultimately, access to care and physician specialists remains one of the most pressing challenges for rural hospitals, leading many to prioritize specialty health and telehealth consults in their strategic applications. To effectively remedy these gaps, it is essential to select a virtual care platform that leverages the specific partnerships necessary to bridge the distance between patients and specialized expertise.
How Can AvaSure Help?
AvaSure’s partnership with Equum Medical, a telehealth-enabled clinical workforce organization, will provide rural hospitals with easy access to virtual specialty consults. The company’s broad portfolio of services addresses the driving challenges of Access and Capacity for health systems, including multi-specialty telemedicine, critical care, virtual nursing, virtual sitter monitoring, and telemetry. Solutions include:
Tele-ICU and critical care support, including surge capacity and after-hours coverage
Virtual hospitalist support for nights, weekends, and hard-to-staff locations
Care coordination that helps reduce avoidable transfers, keep patients local, and support patient flow with integrated virtual nursing capabilities across care venues
These solutions strengthen financial sustainability while offering scalable, broadband-friendly technology specifically designed for the unique constraints of rural settings. Unlike typical telehealth partnerships that add separate point solutions, the integrated model runs on a single platform that many hospitals already use for virtual nursing and patient observation, paired with Equum’s physician and clinical programs.
Your RHTP Virtual Care Strategy
AvaSure equips rural hospitals with innovative virtual care and AI-powered solutions that expand local access, enhance care quality, and strengthen financial sustainability. By reducing adverse events like patient falls, easing workforce burdens, and fostering collaborative models of care, AvaSure helps rural providers meet and exceed the goals of the Rural Hospital Transformation Program.
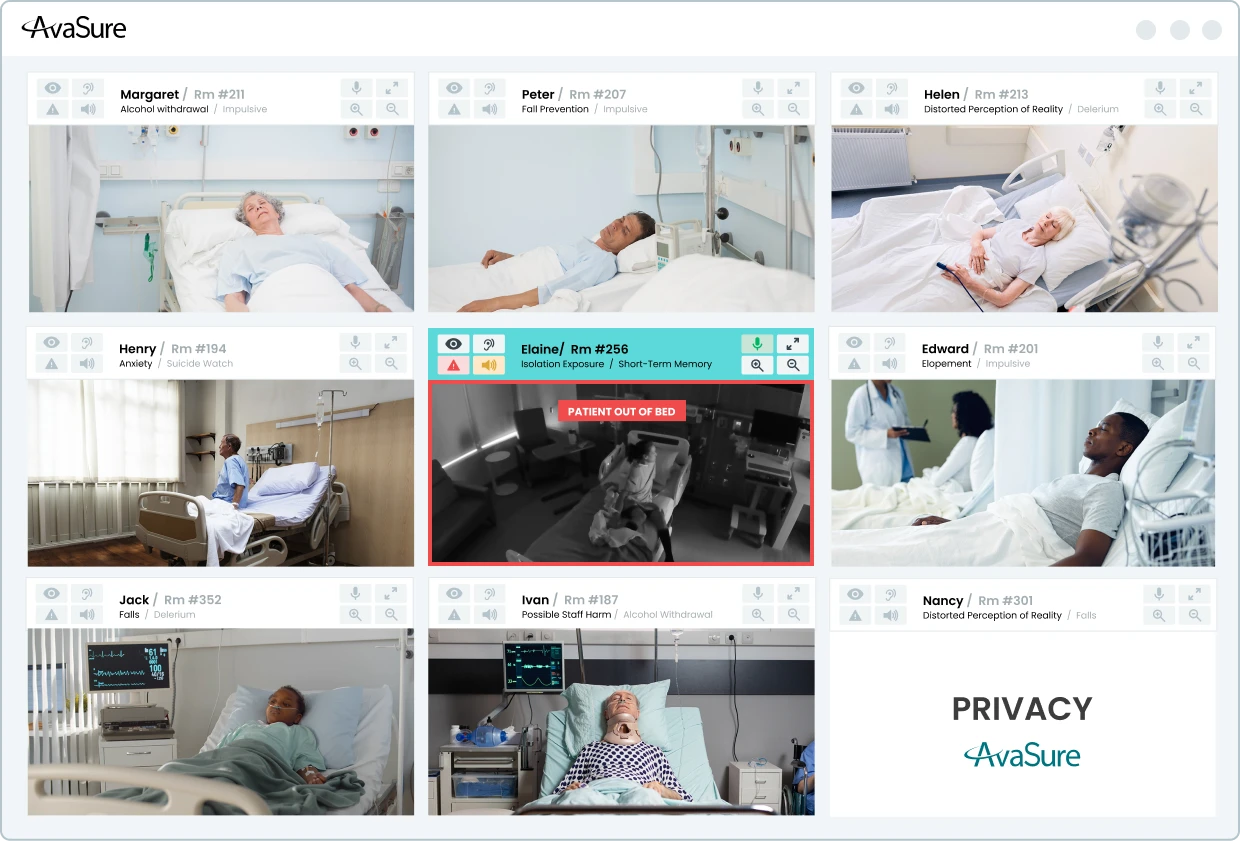
Hospitals are under pressure to reduce preventable harm from falls, elopement, and other adverse events while maintaining a sustainable workload for clinicians. Camera-based monitoring and virtual sitting programs such as AvaSure’s Continuous Observation platform have already demonstrated that continuous observation can reduce falls and injuries, but human-only monitoring does not scale indefinitely. Many organizations are now exploring Artificial Intelligence to extend the reach of their teams, and to detect risk earlier than a human observer might be able to do consistently.
At AvaSure, we view Artificial Intelligence as an extension of the virtual care platform that more than 1,200 hospitals already use for continuous observation, virtual nursing, and specialty consults. Our goal is not to replace human judgement. Instead, we want to build behavior-aware monitoring that can recognize patterns associated with risk, surface those patterns to caregivers in time to intervene, and do so in a way that is technically sound, clinically grounded, and respectful of patient privacy.
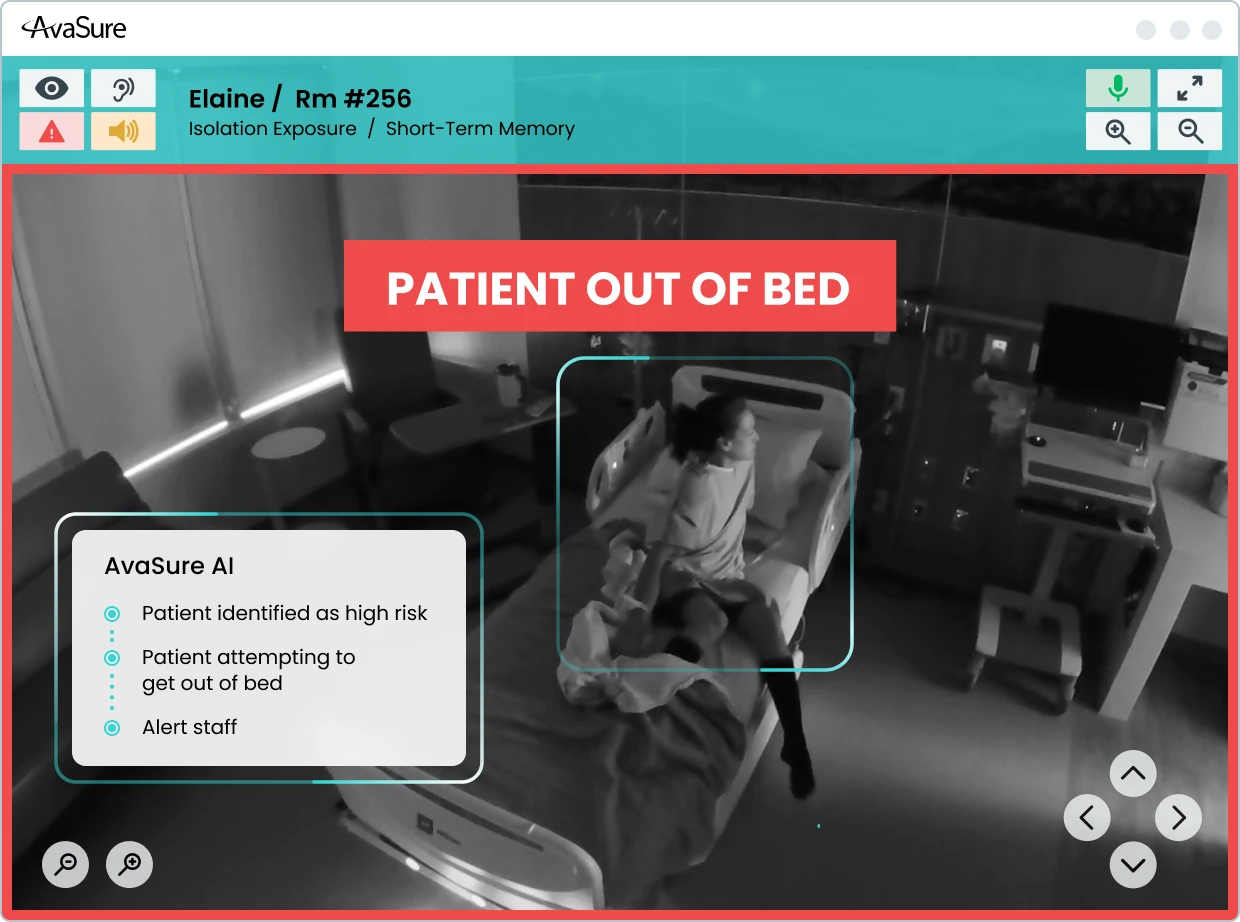
This blog describes the design principles behind our Falls and Elopement Artificial Intelligence system. AvaSure leverages Computer Vision, a subset of Artificial Intelligence, to detect high-risk scenarios before an adverse event occurs. Our Computer Vision models perceive the hospital room environment by learning what situations are unsafe for patients. This allows us to demonstrate the clinical performance of our models made possible by our onboarding process for new hospitals. Built on Oracle Cloud Infrastructure (OCI), this cloud-based system provides a scalable foundation that extends beyond fall and elopement prevention into broader ambient AI applications.
What are the Challenges of Computer Vision Models for Falls and Elopement?
Falls and elopements rarely occur as single, isolated moments. They emerge over a sequence of behaviors. A patient may shift position in bed, sit upright, move to the edge of the bed, stand, and then begin to move away. However, there are challenges to building Computer Vision models that understand such behavior. Staff and visitors come and go, sometimes obstructing the view of the camera. Lighting changes over the course of the day and night, including the use of infrared lighting in low light situations. All these challenges are part of the design space, and a monitoring system that considers a single video frame at a time without regard to such confounding elements can miss much of this context.
An important way to adapt to these challenges is to select the right type of camera device. Choosing the right device for AI for patient safety also impacts how the system perceives the hospital room environment. AvaSure offers a variety of camera devices including Guardian Dual Flex, Guardian Mobile Devices, and Guardian Ceiling Devices. Guardian Dual Flex devices provide a fixed camera dedicated to Artificial Intelligence monitoring. Mobile units introduce variation in pan, tilt, zoom, and location within the room – each of which varies in layout across and within different hospital systems. Guardian Ceiling devices provide a different perspective compared to Dual Flex and Mobile devices.
AvaSure’s Computer Vision system and onboarding processes are built to adapt rather than assuming a single, fixed installation environment. Our current models for Falls and Elopement focus on understanding posture and presence over time while accommodating variations in lighting and environment. The system distinguishes the posture of the patient from lying in bed, sitting on the side of the bed, or standing. These states are evaluated over short time windows and combined with rules that relate them to risk. For example, a transition from lying to sitting on the side of the bed may be treated as an early warning, whereas a transition to standing unassisted may prompt a higher-severity alert.
How Does Falls and Elopement AI Perceive the Patient Room?
The Falls and Elopement models employ a three-layer approach to perceive conditions within the hospital room.
Lowest Layer: Detect whether there are people in the frame and estimate how many.
Middle Layer: When there is a single person in view, form an understanding of posture and location relative to the bed and other furniture.
Top Layer: Combine these posture estimates over time and apply rules that map temporal patterns to alerts.
This layered approach is intentional. Computer vision research has shown that models built only around pose estimation can struggle with common conditions in clinical rooms, such as occlusions from blankets and equipment, low light, and cluttered backgrounds. By combining person detection with semantic posture classification and temporal reasoning, we maintain flexibility in camera hardware while capturing clinically meaningful patterns in the room.
The temporal aspect is central to how the system works. Rather than categorizing each frame in isolation, the models consider short windows of behavior and pay attention to transitions. A single frame showing a patient near the edge of the bed may not be sufficient to decide whether they are attempting to stand or simply shifting position. A sequence of frames that show a consistent movement from reclined to upright to standing is more informative. Alerts are based on this kind of sequence-aware understanding rather than a momentary snapshot.
AvaSure designs for known sources of variability. Mobile cameras introduce changes in viewpoint and zoom as they are repositioned. Different rooms may be arranged in mirror images, with beds and bathrooms on opposite sides. Lighting can range from bright daytime scenes to low-light conditions at night. During model development and onboarding, we deliberately include these variations so that the system can learn to interpret similar behaviors across a range of visual conditions.
How does AI for Patient Safety Learn Real-World Clinical Complexity?
Computer Vision models learn by being fed many examples of different situations. For example, these could be labeled as “a patient lying in bed” or “a patient standing near the side of the bed”. The learning (or training) process then iteratively adjusts the model parameters based on how well the model at that iteration correctly predicts the situation associated with a given example. This process repeats until the model performs well enough. There are several methods for capturing data for training, including having actors stage scenes and having computers generate synthetic scenes by rendering life-like situations.
However, models trained only on staged scenes and synthetic data tend to perform best on those same controlled scenarios. Real hospital rooms are more complex. Patients vary widely in demographic, mobility, and behavior. Equipment is added and removed. Staff and visitors move through the field of view in unpredictable ways. To build models of AI for patient safety that can handle this complexity, we need to learn from images that reflect it. At the same time, patient identity and privacy must be preserved.
AvaSure maintains a patent-pending patient anonymization system that allows us to incorporate real-world imagery into training and evaluation without retaining identifiable visual information. The system applies transformations that remove or obscure personally identifiable features and present them to a human reviewer. The reviewer confirms that anonymization is complete and assigns labels describing the posture and relevant contextual details. Only after this confirmation do the frames enter curated data sets used for training and for measuring performance in production.
The system captures frames concentrated around ambiguous or clinically relevant situations rather than random samples of uneventful periods. This makes them particularly useful for improving model performance for video cases where decisions are hardest.
Precision vs Recall: Which Metrics Matter Most for Clinical Success?
When evaluating models in safety-critical domains, accuracy alone is not sufficient. Falls and elopements are relatively rare events compared with the number of hours of observation across a hospital. A system can achieve high overall accuracy by correctly labelling long periods of low-risk behavior yet still miss important events or generate more alerts than staff can reasonably handle.
For this reason, AvaSure frames performance in terms that reflect the realities of clinical operations. Precision captures how often an alert corresponds to a meaningful event. Recall captures how often the system detects an event when it occurs. The F1 score combines the two into a single measure that balances false positives and missed detections. These metrics tell us how often the system asks for attention when it is truly warranted and how often it remains silent when it should speak up.
In practice, different hospitals and units may prefer different trade-offs. A neurosurgical ward may choose to tolerate more alerts in exchange for fewer missed events, whereas a lower-acuity unit may prioritize reducing unnecessary interruptions. Our models can operate at different points along the precision-recall curve, and part of the onboarding process is to discuss and tune that operating point together with clinical and operational leaders.
Beyond the initial deployment, AvaSure treats performance as something that must be monitored and maintained. As room layouts, staffing patterns, and patient populations change, the distribution of behaviors the system sees will change as well. By sampling outputs in the field for new models running side by side with existing models, we can compare new model versions against established baselines and roll back changes that do not meet defined criteria.
Deployment Without Disruption: What is the Process for Onboarding New Hospitals with AI for Patient Safety?
For hospitals, the most important questions are how the system will behave in their specific environment and how disruptive deployment will be. AvaSure’s onboarding process is designed to answer those questions incrementally and transparently.
The work begins with understanding room configurations, typical camera locations, and the kinds of patients and use cases each unit expects to monitor. This can include having AvaSure team members stage representative scenarios in sample rooms, capturing video that reflects local layouts, lighting, and camera angles. This staged data helps verify that the baseline model behaves as expected before any live patient feeds are involved.
As cameras are connected, we run the models in background mode. The system processes live video, but alerts are not yet sent to staff. During this period, we collect anonymized frames of interest and review the patterns of potential alerts. This is also when we fine-tune the operating point where we can adjust the precision vs recall for the unit’s needs.
Once the hospital is comfortable with the system’s behavior, alerts are enabled for virtual safety attendants. The user interface will increasingly support structured feedback so that attendants can indicate whether an alert was helpful, spurious, or associated with an event the system should have recognized. These feedback signals, together with anonymized frames, feed back into our data and model improvement process. By gathering room dimensions, lighting, and arrangement details, we are able to use rendered scenes that are specific to each environment, streamlining the creation of training examples for new hospitals.
How to Extend Beyond AI for Patient Safety Monitoring
Falls and elopements are a natural starting point for behavior-aware monitoring because they are common, clinically important, and directly connected to existing continuous observation workflows. However, the same sensing and inference capabilities can support a broader set of safety and quality use cases over time.
AvaSure’s AI Augmented Monitoring strategy anticipates an expansion from Falls and Elopement into additional use cases such as hospital-acquired pressure injury prevention, infection-related behaviors, and staff duress. Environmental sensing capabilities, including detection of meal tray delivery and removal or patterns of in-bed movement, can contribute to these use cases by providing objective, continuous signals about patient status and care processes. Each new application will require its own feasibility studies, data collection plans, and validation steps, but they build on the same underlying platform and design approach.
Each of these additional use cases requires enhancements to the Computer Vision models to have them comprehend a wider variety of situations. Such enhancements can require additional or more complex models requiring additional computing power. AvaSure leverages OCI’s AI infrastructure offerings to bring to bear considerable GPU-powered computing to support an expanding range of use cases.
How do we integrate security and compliance into the design of healthcare AI models?
Security for us is not a separate track from Artificial Intelligence; it is part of the design of the platform and the models from the beginning. AvaSure’s virtual care systems already operate in environments where SOC 2 and HIPAA expectations are the baseline, not an add-on, and the same standard applies to AI Augmented Monitoring. Every new service that touches patient data, from model pipelines to anonymization computing, is expected to pass formal design review, threat modelling, and, where appropriate, penetration testing before it is considered ready for production.
At the infrastructure level, our cloud strategy is built on a scalable, multi-tenant architecture designed to keep different users and services securely separated. Robust identity and access management ensures that only authorized components can communicate or access sensitive data, and every service operates with the minimum permissions required. Data moving through the system is protected by encryption, as is data stored in managed services. Comprehensive audit logging is a core part of our approach, recording authentication and authorization events, configuration updates, model changes, and administrative actions so that security and compliance teams can thoroughly review activity if needed.
For AI specifically, the same security-by-design approach applies. Security specialists review designs for new AI use cases during ideation rather than waiting for prototypes. The review looks at how video streams enter the system, where inference is performed, what outputs persisted, and how PHI is handled or removed. This helps ensure that the introduction of GPU-backed inference or new data flows does not inadvertently expand the attack surface or weaken isolation guarantees.
The anonymization pipeline is an example of security and privacy concerns shaping the technical design. Rather than storing raw patient video, the system extracts short windows around events of interest and routes them to a separate anonymization service. That service applies privacy preserving transforms and requires human confirmation that identifiable information has been removed before frames can be used for training or evaluation. All of this traffic is encrypted in transit; anonymized images are encrypted at rest and stored with restricted access. This architecture allows the models to benefit from realistic data while maintaining clear boundaries around PHI.
In practice, ensuring security involves closely connecting monitoring activities with incident response protocols. A comprehensive strategy includes full observability across systems and processes, using tools like metrics, alerts, dashboards, and health checks to quickly detect and respond to any unusual activity. The same mechanisms that support autoscaling and automated rollback for availability also support security; if a change in configuration or dependency were to introduce unexpected behavior, operators can detect it quickly and revert. Regular risk assessments, combined with continuous integration and deployment practices, are intended to keep the platform aligned with evolving threats and regulatory expectations rather than treating compliance as a static checklist.
From the hospital’s perspective, the outcome of this approach should be straightforward: AI features sit inside a platform that is already held to enterprise security and compliance standards, and any new capability is expected to meet those standards before it is offered in production. The same controls that protect virtual care today – access control, encryption, audit logging, and formal review – apply equally to behavior-aware monitoring and future AI use cases.
How Does AvaSure Scale AI for Patient Safety in Modern Health Systems?
Building AI for patient safety is not simply a matter of choosing a model architecture or training on a large data set. It is a system-level effort that spans model design, data collection, anonymization, infrastructure, onboarding, monitoring, security, and governance. Each part influences how the technology behaves in practice and how much clinicians and patients can rely on it.
For AvaSure, the core elements of that system are clear. We focus on understanding behavior in context rather than isolated frames. We adopt a stepwise development approach that involves staged experiments, demonstrations, and validation in real clinical settings. We learn from real rooms through an anonymization data collection system that protects identity while concentrating on data where it matters most. We operate on a cloud platform designed for reliability, scalability, and security. Lastly, we treat hospitals as partners in an ongoing improvement process rather than one-time installations.
AvaSure is building AI for patient safety into the virtual care platform that customers already use for continuous observation and virtual nursing. Future blogs will explore specific components in more depth, including anonymization and data curation, our hybrid edge–cloud roadmap, and the evolution from single-use models to a suite of AI augmented monitoring applications. For now, our aim is to make the underlying approach visible so that hospital leaders and clinicians can make informed decisions about how AI fits into their own patient safety strategies.
In recent history, no technology has so quickly penetrated the cultural zeitgeist as artificial intelligence (AI). At an ever-increasing pace, AI is being hailed as a transformative force capable of revolutionizing industries worldwide, and healthcare is no exception. Companies across the globe are racing to utilize AI to automate, simplify, and rationalize manual tasks across every sector, recognizing its potential to solve some of the most persistent, existential challenges facing modern healthcare systems.
For years, healthcare has grappled with tremendous cost pressure, chronic staffing shortages, and an overwhelming administrative burden contributing to high rates of clinician burnout. Hospitals have focused on utilizing technology to drive significant change through the digitization of documentation, consolidation of health systems, and the virtualization of traditional care models. However, often these tools – while helpful -have not delivered the seamless simplicity, actionable insights, or scale necessary to alleviate the core pressures.
The integration of AI, particularly into technologies like intelligent virtual care platforms, represents a critical shift. It moves us beyond mere digitization to intelligent automation. This guide delves deeply into the capabilities, benefits, challenges, and practical steps necessary for healthcare organizations to effectively harness the power of AI, transforming it from a passing technology trend into a reliable foundation for the future of patient care.
The Core Technologies Driving AI in Healthcare
The umbrella term “Artificial Intelligence” encompasses several distinct technologies, each with unique applications in a clinical setting. To understand how AI can reshape patient care, it is essential to explore these core components in depth.
What is Machine Learning (ML) and Deep Learning?: The Engine of Modern AI
Machine Learning is a subset of AI where systems learn from data, identify patterns, and make decisions with minimal human intervention. Deep Learning, a more advanced form of ML, utilizes artificial neural networks with multiple layers to process complex data, like medical imaging, genomic sequences, or patient physiological data, allowing for highly sophisticated pattern recognition.
Real-World Application: ML models are primarily used in diagnostics and risk stratification. For example, Deep Learning algorithms can be trained on millions of historical electrocardiograms (ECGs) to detect subtle, early signs of atrial fibrillation or myocardial infarction that a human eye might miss. Similarly, in genomics, ML helps identify genetic markers that predispose a patient to certain diseases, paving the way for truly personalized medicine.
What is Natural Language Processing (NLP)?: Transforming Unstructured Data
Healthcare data is notoriously messy. A vast majority of critical patient information – physician notes, discharge summaries, radiology reports, and dictated records – is locked away in unstructured text formats. Natural Language Processing (NLP) is the branch of AI that enables computers to understand, interpret, and generate human language.
In-Depth Use Cases:
Clinical Documentation: NLP converts free text or speech into structured data, automatically populating electronic health records (EHRs). This drastically reduces the time clinicians spend on administrative tasks.
Sepsis Detection: Advanced NLP algorithms can scan unstructured notes in the EHR, looking for phrases like “patient looks pale,” “fever spiking,” or “lactic acid elevated,” and combine this with structured data to generate an early warning score for sepsis, often hours before traditional systems would flag the risk.
Information Retrieval: NLP allows researchers and clinicians to query massive datasets of patient records, finding patterns in treatment efficacy and outcomes that would be impossible to manually extract.
What is Conversational AI and Virtual Assistants?: Bridging the Communication Gap
Conversational AI uses a combination of NLP, machine learning, and dialogue management to enable human-like interactions. In healthcare, this manifests as chatbots, virtual assistants, and intelligent patient portals.
Patient-Facing Applications:
Triage and Scheduling: AI chatbots can handle initial patient queries, symptoms assessments, and guide patients to the appropriate level of care, or automatically schedule appointments, significantly reducing the workload on call centers.
Patient Education and Support: Post-discharge, AI can send automated, personalized check-ins and educational content tailored to the patient’s specific condition, ensuring adherence to recovery plans and monitoring for red-flag symptoms.
Medication Reminders: Virtual assistants can provide timely reminders about medication adherence, which is crucial for managing chronic diseases.
Why is Predictive Analytics Important? Forecasting Health Outcomes
Predictive analytics mines vast amounts of aggregated data, including patient history, real-time physiological metrics, environmental factors, and demographic information to plug into algorithms that project future events or risks.
Key Applications in Risk Mitigation:
Readmission Risk: Hospitals use predictive models to flag patients at high risk of readmission within 30 or 90 days of discharge, allowing care coordinators to intervene proactively with resources, patient education, or follow-up appointments.
Sepsis and Cardiac Arrest: By continuously analyzing streaming patient data from monitors and EHRs, predictive analytics can generate real-time risk scores, giving care teams precious hours to intervene before a life-threatening event occurs.
Population Health: For public health, predictive models forecast disease outbreaks, hospital capacity needs, and resource allocation requirements during crises like pandemics.
What is Computer Vision and AI-Powered Imaging?: Enhancing Diagnostics and Safety
Computer Vision (CV) is the technology that enables AI systems to derive meaningful information from digital images, video, and other visual inputs. Its application in healthcare is rapidly expanding from the laboratory to the bedside.
In-Depth Use Cases:
AI-Powered Imaging Diagnostics: CV algorithms are trained to analyze medical images (X-rays, CT scans, MRIs, pathology slides) to detect subtle anomalies that may indicate early-stage disease. A critical real-world example is the use of AI tools to rapidly identify pulmonary nodules in CT scans or to flag microcalcifications in mammograms, enabling earlier detection and treatment of lung and breast cancer.
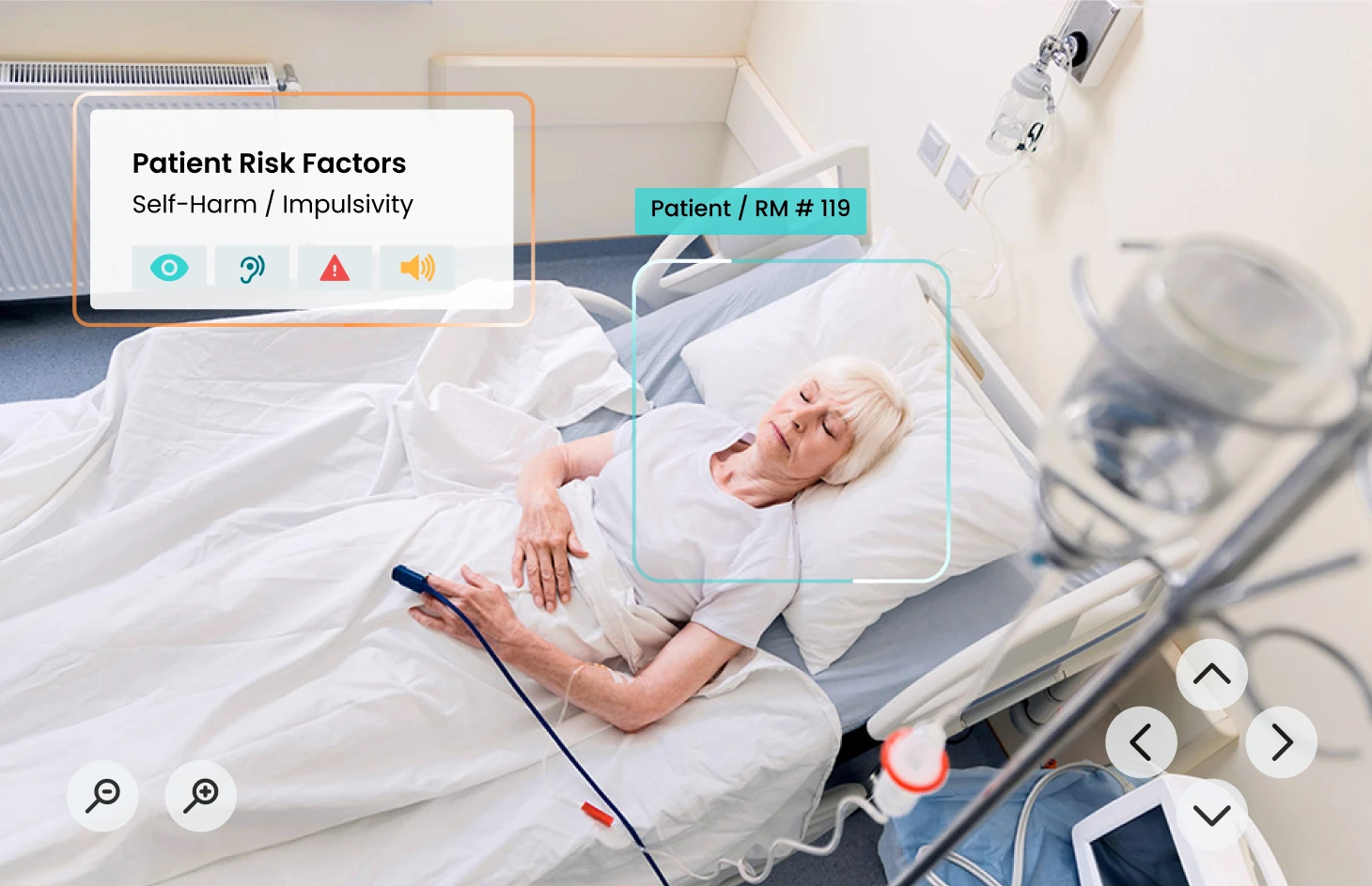
Patient Safety Observation: At the bedside, sophisticated CV systems embedded in virtual care devices like the AvaSure platform monitor patient movement in real-time. These systems can identify high-risk behaviors, such as a patient attempting to climb out of bed or a visitor violating isolation protocols, and issue immediate, actionable alerts to a remote observer. This proactive monitoring dramatically reduces the occurrence of Never Events like patient falls and the development of hospital-acquired pressure injuries (HAPIs) by intervening before injury occurs.
Why Ambient Listening is Important: Alleviating Clinician Burden
Ambient listening technology uses microphones to capture conversations, typically between a patient and a clinician, and then employs NLP to transcribe and structure the content. This is distinct from NLP in that it is designed for a live, real-time clinical encounter.
Use Case: Clinical Scribing: The primary application is to automatically draft clinical notes. Instead of typing into the EHR during or immediately after an encounter, the clinician can focus entirely on the patient. The AI listens, captures key phrases like medical terms, diagnoses, orders, and action items, and populates the patient’s chart, saving hours of administrative time and directly combating clinician burnout.
AI’s Direct Impact: What are the Benefits of AI for Patients and the Patient Experience?
While much of the early AI focus centered on efficiency and cost savings for hospitals, the most profound impact of this technology is on the patients themselves: improving safety, quality of life, and the overall healthcare experience.
Personalized Medicine and Treatment Planning
AI’s ability to process complex, multi-modal data is the backbone of precision medicine. By integrating a patient’s genomic data, electronic health record, lifestyle information, and even wearable device data, AI can create a highly detailed, predictive portrait of their health. This allows physicians to:
Tailor Drug Dosing: Determine the exact medication and dosage that will be most effective for a patient based on their genetic makeup, minimizing adverse reactions.
Optimize Treatment Paths: Predict how a patient’s cancer will respond to specific chemotherapy or radiation protocols, adjusting the plan in real-time based on AI-driven feedback loops.
A hospital stay can be confusing and stressful. AI-powered virtual assistants are beginning to serve as in-room digital concierges, empowering patients and reducing the need for non-clinical nursing interruptions.
Simple Request Fulfillment: Patients can use voice commands or a tablet interface to request essential, non-urgent services, such as a blanket, a meal menu, or adjustment of room temperature, which are then automatically routed to the appropriate department.
Information Access: The virtual assistant can answer common questions about the hospital facility, discharge procedures, or medication schedules, providing instant information and reducing the burden on clinical staff.
Personalized Patient Education and Engagement
General patient handouts often fail to resonate. AI can dynamically generate educational content that is tailored to a patient’s:
Health Literacy Level: Adjusting complexity and vocabulary to ensure understanding.
Specific Context: Focusing education on the exact medications or procedures the patient has undergone.
Preferred Language: Offering information in native languages, improving comprehension and adherence.
How Do You Expand Access with AI in Telemedicine Services?
AI is fundamentally changing the delivery model of telemedicine, allowing for remote care to be more sophisticated and scalable.
Virtual Nursing Support:Virtual Nursing programs leverage remote clinicians to assist with tasks like admissions, discharges, medication reconciliation, and patient education. AI enhances this by identifying which patients require an immediate virtual check-in based on real-time risk scores and physiological data, allowing remote nurses to prioritize their attention to where it is needed most.
Remote Diagnostics: AI-enabled tools allow general practitioners in rural settings to upload specialized images or data (e.g., dermatological pictures or retinal scans) that are instantly analyzed by AI for preliminary diagnosis before being sent to an off-site specialist for final review.
Navigating the Complexities: What are the Challenges and Ethical Considerations of AI?
The transformative potential of AI is matched by significant challenges, particularly concerning ethics, data, and regulatory oversight. Ignoring these issues risks undermining the very trust AI is intended to build.
The Critical Need for Trust and Transparency (Explainability/XAI)
One of the most persistent issues in AI is the “black box” problem. Many sophisticated deep learning models are so complex that even their designers struggle to articulate why a particular decision was made. In healthcare, where decisions can be life-altering, this lack of data interpretability is unacceptable.
Explainable AI (XAI): The imperative is to develop XAI tools that can not only provide a diagnosis or risk score but also show the underlying data and logic used to arrive at that conclusion. Clinicians need confidence in the tool, and patients deserve to know why a treatment path was recommended.
Validation of AI Models: Before deployment, every AI model must undergo rigorous validation using external, real-world data sets to ensure it performs accurately and consistently across diverse patient populations.
Validation, Verification, and the Risk of Hallucinations
AI systems, particularly large language models (LLMs) used in conversational AI, are susceptible to hallucinations – generating plausible-sounding but factually incorrect information. In a clinical context, a hallucination could lead to a catastrophic medical error.
Verification: Implementing AI systems requires robust verification loops, ensuring that AI-generated clinical notes, suggested diagnoses, or treatment plans are always reviewed and approved by a qualified human clinician before execution.
Model Drift: Healthcare systems must continuously monitor AI performance because models can “drift” over time as new patient data or clinical protocols emerge, making the original training data less relevant.
Addressing Bias and Ensuring Ethical AI Decisions
AI is only as objective as the data it is trained on. If a training dataset over-represents one demographic (e.g., white, male, high-income patients) and under-represents another (e.g., minority, low-income, geriatric patients), the resulting AI model will be inherently biased.
Health Equity: Deploying biased AI systems can exacerbate existing health inequities by systematically under-diagnosing, over-diagnosing, or recommending suboptimal treatment for under-represented groups.
Ethical Implications of AI Decisions: Organizations must establish clear guidelines for when an AI’s recommendation can be overridden, who is accountable when an AI decision leads to an adverse event, and how the system promotes fairness and equity in access to care.
Regulatory Hurdles and Data Governance
The deployment of AI tools that actively influence diagnosis and treatment requires stringent regulatory approval, typically from the FDA. Unlike a software update, a change to the AI model itself may require a new review. Furthermore, data governance is paramount:
HIPAA Compliance: All healthcare AI must adhere to strict privacy regulations (like HIPAA in the US) regarding the collection, storage, and processing of protected health information (PHI).
Data Security: AI requires massive amounts of data, making the security of these large repositories a top concern to prevent breaches and maintain patient trust.
A Practical Roadmap: How Do You Implement AI in Healthcare Organizations?
The adoption of AI should not be a scramble for the latest gadget, but a deliberate, strategic investment. Healthcare organizations need a practical, stepwise approach to implementation to maximize return on investment and clinical benefit.
Stepwise Adoption: Aligning Needs and Goals
Paul White, Distinguished AI Engineer for AvaSure reminds us, “It is important to take a stepwise approach to adoption. Many companies are rolling out AI solutions geared towards creating new efficiencies or solving different issues within the hospital setting. Therefore, the first step should be identifying companies that are building AI solutions that address most crucial areas of need.”
The initial phase must focus on organizational readiness and strategic alignment:
Assess Readiness: Evaluate existing IT infrastructure, data governance protocols, and the quality of historical data. AI relies on clean, accessible data.
Identify Crucial Areas of Need: Do not implement AI just for the sake of it. Where are the organization’s most acute pain points? Is it staff retention, patient falls, sepsis mortality, or long wait times? The AI solution must directly address a high-priority problem.
Define Success Metrics: Clearly define what success looks like before implementation (e.g., “Reduce patient falls by 50% in the first year,” or “Decrease time spent on charting by 2 hours per nurse per shift”).
Prioritizing Use Cases for Maximum Impact
Once organizational needs are identified, organizations can align those needs with the AI technology that offers the most immediate, tangible solution.
Example 1: Addressing Clinician Burnout
Need: Excessive administrative burden, high EHR time.
AI Solution: Leveraging AI Clinical Documentation/Scribing solutions (Ambient Listening/NLP) is a great choice for alleviating administrative burden and allowing clinicians to refocus on patient care.
Example Two: Mitigating Never Events
Need: High incidence of falls, Hospital-Acquired Pressure Injuries (HAPIs), Hospital-Acquired Infections (HAIs).
AI Solution: Partner with Virtual Care companies leveraging computer vision to mitigate the occurrence of these events. AI monitors the patient’s room 24/7, detects high-risk actions (e.g., a patient reaching for a line), and alerts a remote observer before the patient falls, turning reactive care into proactive prevention.
Build, Buy, or Partner?
A critical strategic decision is whether to develop an AI system internally or acquire a solution from an external vendor.
Build (Internal Development): Requires massive internal investment in data scientists, ML engineers, and clean training data. This is typically only feasible for the largest health systems with deep research capabilities.
Buy (Vendor Solution): The most common path. Healthcare organizations can purchase validated, ready-to-deploy solutions. Paul White adds,“It is crucial to understand and align with a vendor whose ethos matches your own.” Look for vendors who demonstrate a commitment to:
Clinical Validation: Providing proof of concept and third-party validation studies.
Seamless Integration: Ensuring the AI solution integrates smoothly with existing EHRs and virtual care infrastructure.
Ethical AI: Showing commitment to transparency, minimizing bias, and data security.
Change Management and Clinician Buy-in
No matter how powerful the technology, AI implementation will fail without clinician support. The fear that “AI will replace my job” must be addressed head-on.
Focus on Augmentation, not Replacement: Position AI as a “co-pilot” or intelligent assistant that removes tedious tasks, enhances diagnostic capability, and reduces cognitive load, allowing clinicians to practice at the top of their license.
Training and Workflow Integration: Training should focus less on the technology of AI and more on how it seamlessly fits into and improves the existing clinical workflow.
Looking Ahead: What are the Future Trends of AI in Healthcare?
The integration of AI into healthcare is not an end point, but the beginning of a new era of medical practice. The next decade promises even more radical transformation.
Deeper Integration of Virtual and In-Person Care
Anticipated technological advancements will blur the lines between virtual and physical care:
Ubiquitous Sensors: Low-cost, non-invasive sensors (wearables, smart textiles, in-room monitoring) will feed continuous, high-fidelity physiological data into AI systems.
Closed-Loop Automation: AI will move beyond alerts to initiating automated actionsfor example, automatically adjusting IV pump rates based on real-time blood pressure data, or using an in-room virtual care platform to deliver a two-minute therapeutic intervention immediately after a patient is flagged as high-anxiety.
The Era of Tech-Healthcare Collaborations
The future will be defined by strategic partnerships between leading technology firms (Google, Microsoft, NVIDIA, etc.) and pioneering healthcare organizations. These collaborations are essential because tech companies bring computational power and AI expertise, while healthcare partners bring critical, proprietary clinical data and workflow knowledge. This synergy will accelerate the development of lifesaving, regulated AI solutions.
AI as a True Co-Pilot for Healthcare Delivery
In the long term, AI will function as a true co-pilot for every member of the care team:
For Radiologists: AI systems will triage scans, flagging critical cases and providing initial measurements, allowing the human expert to focus their attention and time on complex diagnoses.
For Surgeons: AI will assist in pre-operative planning, intra-operative guidance using computer vision for precision, and robotic assistance, leading to safer, more reproducible outcomes.
For Nurses: AI-enabled virtual care will handle many of the repetitive safety checks and administrative tasks, allowing nurses to spend their time at the bedside engaging in therapeutic communication, complex problem-solving, and providing the essential human touch that AI can never replace.
Conclusion: Fact vs. Fiction
AI is no longer a futuristic concept; it is a present-day reality that is already driving efficiency and saving lives. The technologies, from Machine Learning diagnostics to Computer Vision patient safety platforms, are primed for widespread adoption. By taking a thoughtful, stepwise, and ethically sound approach to implementation, healthcare organizations can ensure that they are not just adopting a new technology, but building a more resilient, efficient, and patient-centric healthcare system for the next generation.
To learn more about the reality of AI adoption in the clinical setting, watch our Webinar featuring Aaron Miri, Senior VP and Chief Digital and Information Officer of Baptist Health and Elizabeth Gunn, VP of Patient Services for Baptist Medical Center South: AI in Healthcare: Fact vs. Fiction
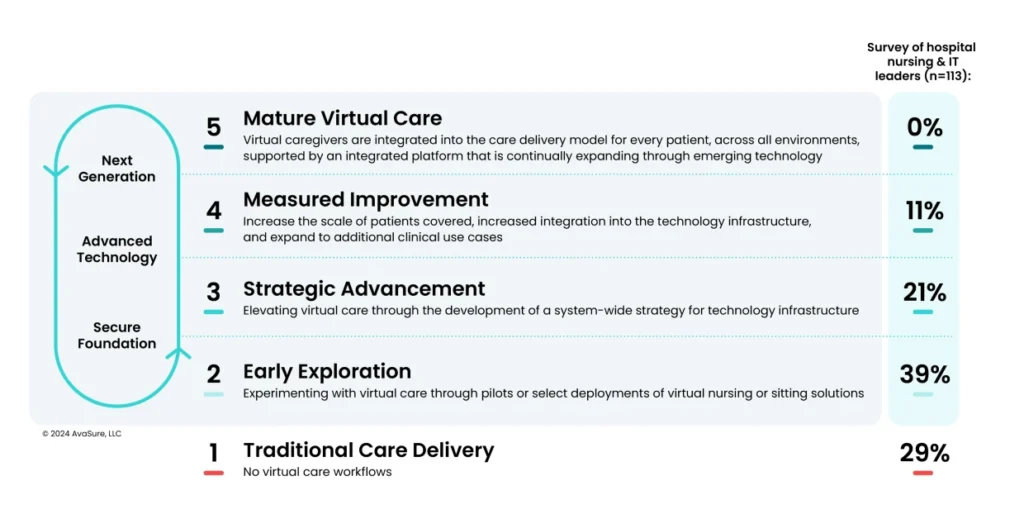
Industry experts, healthcare leaders & the market have all agreed – virtual nursing is here to stay. In a 2024 study, 74% of hospital leaders reported that virtual nursing will become integral to care delivery models in acute inpatient care —up from 66% in 20231. However, only 10% of hospital leaders have reached a phase where virtual care is a standard part of care delivery, and nearly 30% of hospitals have no virtual care workflows at all1.
Why the gap?
Pilot or partial deployments of virtual nursing are where most institutions are getting stuck!
How can we break through perpetual pilots and scale virtual nursing to be a standard part of care delivery?
Let’s ask the experts.
AvaSure, a leading provider of Intelligent Virtual Care Platforms, consulted with two leading healthcare institutions that have successfully moved beyond the pilot phase and fully integrated virtual nursing into their daily patient care. Together, they explored how these organizations made the transition and shared valuable insights and advice for other institutions just beginning their virtual nursing journey.
UCHealth, a nationally recognized healthcare system with $7.5 billion in operating revenue and over 33,000 employees, operates 14 Colorado hospitals, providing more than 2,500 inpatient beds, and over 200 clinics across Colorado, southern Wyoming, and western Nebraska. Their 2016 Virtual Health Center significantly enhances patient care through virtual deterioration monitoring, TeleICU, centralized telemetry, virtual admission & discharge support, virtual sitting, virtual consults & more. This Virtual Health Center has touched over 2.3 million patient lives, achieving remarkable outcomes like reducing code blue rates by up to 40%, increasing rapid response rates and improving patient safety through virtual sitting, yielding nearly $9 million in 1:1 sitter cost savings. To support these expanded use-cases and future-proof the patient room for a hybrid patient care model, UCHealth implemented a ‘camera-in-every-room’ philosophy.
Amy Hassell, MSN, BSN, RN, CNO of Virtual Health Center, UCHealth
Tamera Dunseth Rosenbaum, DNP, RN, NE-BC, System CNO of UCHealth
As New Jersey’s largest and most comprehensive not-for-profit healthcare network, Hackensack Meridian Health (HMH) delivers a full spectrum of medical services, innovative research, and life-enhancing care through its 18 hospitals, 36,000+ team members, 7,000 physicians, and 500+ patient care sites. HMH kicked off their virtual nursing journey in 2022 with the goal of improving outcomes and patient/provider satisfaction. With a virtual nursing pilot focused on virtual admission & discharge support, they successfully removed time-consuming task-based work from bedside teams. Following a year of successful implementation, the results prompted hospital leadership to expand the program across four hospitals.
11.6% reduction in length of stay
65% reduction in RN traveler hours and 26% reduction in RN overtime hours
0.68% reduction in readmission rates
Marie Foley-Danecker, DNP, RN, CCRN, NE-BE, Vice President & Chief Nursing Office of Hackensack Meridian Health
Pilot sticking point: Lack of organizational alignment on program goal requires vision & change management
Lesson One: It requires both leadership support and buy-in from frontline staff to be successful.
The true blending of virtual and in-person clinical workflows is a technology investment, a change in nursing practice and a change in patient care – so “don’t underestimate the amount of cross-functional alignment it takes to get to one platform, one operating strategy across the network – it takes a village,” said Marie Foley-Danecker. HMH has 5 distinct project teams that stood up to help scale their pilot across the system:
Tech Build Team (Both Network and Site Level) – make decisions around hardware, software, server, infrastructure, hosting and more – ensuring the system has not just the right technology, but the support infrastructure needed to support ongoing virtual care.
Clinical Workflow Team – help to ensure that bedside workflows are standardized and the virtual workflows fit seamlessly into them. If you don’t start with standard work at the bedside, it will be nearly impossible to add a virtual care workflow.
Nursing Operations Team – help manage staffing, define roles & responsibilities between team members and drive collaboration
Education Team – ensure the internal education of facility teams, as well as patients & family members so that they understand the role of the virtual care team members in their visit
Communications Team – tackle marketing and promotion of the program externally, helping to improve the hospital’s reputation as a cutting-edge, patient-experience oriented site of care. Robust virtual care programs can also act as great recruitment tools for future nurses who want to work at systems investing in the latest technology.
Lesson Two: Prepare for and be willing to adapt quickly.
“Be nimble and understand that you might not get it right, right out of the gate. That’s why having a governance structure (like the teams at HMH or a steering committee approach at UCHealth) that can be quick to identify issues and change processes is really important” said Tamera Dunseth Rosenbaum. It’s essential to remember the primary reason why you’re doing this – to provide support to your bedside teams. So, listen to them! Be sure to take in their ideas of what may help and lean into those ideas. Example: HMH, at the suggestion of front-line teams and following suit of many facilities, chose to start with admission & discharge as their first virtual nursing use case. Bedside team members see a lot of value in the ability to offload task-based, administrative work to virtual teams in order to give them more time for hands-on patient care. Furthermore, virtual care team members who are focused specifically on admission & discharge – or other task-based nursing work – can be hyper focused, resulting in spending more time connecting with the patient and often seeing better results. A true win/win! Similarly, UCHealth chose to utilize the virtual nurse answer and triage call lights as a part of their first use case. However, it quickly became apparent that this was adding burden to the bedside with unnecessary steps and communication overload. They took note, quickly changed course, and have since seen greater success. This willingness to adapt & change will be critical to the success of any virtual care program – and to winning the support of your team.
Lesson Three: Build grassroots support.
The bedside team is critical for program success, so giving them a voice is essential. If you don’t know where to start, listen to your front-line nurses – and think about what would make their lives easier. Selecting a first use case that directly benefits them will help with long-term program success. As you get to more complex use cases, like TeleICU, virtual deterioration monitoring, TeleStroke and more, trust between virtual and bedside teams will be vital. You can build this trust through making front-line nurses feel a part of the implementation, ideation, and ongoing governance of the virtual nursing program.
Pilot sticking point: staffing the program
Many facilities are already struggling with the chronic staffing shortage, so how do you find the staff for a virtual nursing program? There are two main paths – utilize your existing talent pool to fill virtual roles or work with a staffing partner who can help provide the adequate staff for your program. Let’s discuss each model & the pros/cons of each.
Utilizing your existing talent pool
Tips & things to consider:
Keep job descriptions consistent between on-site and virtual: This allows for flexibility for floating or job sharing between bedside and virtual roles, without creating unnecessary HR hurdles. Also, offering a virtual shift can be a nice benefit to bedside team members – facilities use this to reward seniority, help prevent burnout and improve staff satisfaction.
Think outside your geography: The nursing shortage is more acute in certain regions. For example, HMH, located in New Jersey, knew that finding nurses in this expensive, metropolitan area would potentially prevent getting their program off the ground. In this instance, working with a partner based out of Tennessee with a richer talent pool, like Equum Medical, made sense for avoiding staffing restraints that would prevent them from getting their program started.
Evaluate the experience level of your current staff: If your facility is predominantly novice nurses, you’ll need your most experienced nurses at the bedside to make virtual care a success. Pulling these nurses into virtual roles could potentially increase travel nurse/overtime use, offsetting potential program ROI. In these cases, outsourcing with a staffing partner may be a better fit for your institution.
Working with a virtual staffing provider
Tips & things to consider:
Speed to go-live: Outsourcing to a trusted provider of virtual nurse staffing may allow you to get started quicker, as they have teams ready to deploy immediately. You can always consider moving things in-house overtime once your program is scaled.
Add more use cases with supplemental staffing: Staffing doesn’t need to be all in-house or all partners! You can take a use case driven approach and use a staffing partner to fill gaps in your team’s experience. Outsource staffing for more complex use cases, like virtual patient deterioration or TeleICU.
Important insight: Marie Foley-Danecker said, “trust is earned—whether you choose to use a partner or have your own staff on the virtual team, the beside team will take time to trust them. Don’t assume that trust will be built immediately just because you use your own staff, or assume trust can’t be built if you outsource.”
Pilot sticking point: funding the program
One of the most talked about reasons for the lack of virtual nursing adoption is the funding. Like many things, leaders struggle to build the business case to pay for it. Some have a misconception that only affluent health systems, or those with a highly favorable payor mix, can afford it. However, HMH and UCHealth both have a challenging payor mix across their system and had to work hard to validate the business case to leadership. Some of their lessons learned include:
Allocating virtual nurse resources to each department.
UCHealth accomplishes this by allocating a small unit of service bump to each department that utilizes the virtual resource. At the care unit level, it can be as small as 0.1 – 0.2 hours per patient day, but UCHealth recommends this path for a few reasons:
Encourages use of the virtual team – if the department is “paying for it anyways”, they’re more likely to utilize the virtual team, helping to improve program utilization.
Helps to spread the cost and avoid constant justification to hospital leadership – When the entire virtual care program is consolidated under a single budget, it becomes a frequent target for scrutiny during budget reviews. Spreading the allocation makes it less likely to face ongoing questioning or review.
Tip: Be sure to have the virtual resource as a separate line item on each nurse manager’s budget to remind them that this is the FTE for the virtual team support. Otherwise, they may hire up to that amount, and the program will be over budget.
Hits budgetary targets – With turnover and vacancy rates most departments can still hit their budgetary targets with this allocation.
Labor savings from virtual sitting can help fund investment in devices for other use cases – like virtual nursing.
Both UCHealth and HMH began their inpatient virtual care programs with virtual sitting. The program was focused on reducing labor costs associated with 1:1 sitters and preventing patient falls. Virtual sitting is a mainstream nursing intervention proven to help facilities replace an average of 70% of 1:1 sitters while reducing falls rates by up to 60%. UCHealth has saved $9M in labor costs with virtual sitting achieving up to 6x ROI. Facilities can utilize these labor savings to help fund the investment in a virtual care device for every patient room.
Pilot sticking point: sufficient infrastructure & technology
Medical quality audio and video devices are fundamental to enable virtual care workflows. Many pilots rely on mobile carts or tablets as a small proof of concept. However, this makes it challenging to scale as it creates additional workflow challenges that impact program success. Because of this, both UCHealth and HMH now standardize patient rooms with a device included and would recommend the same to anyone considering full-scale virtual nursing. This doesn’t mean you always need to add an additional vendor to your portfolio, as this can be a pain point for IT leaders constantly tasked with vendor consolidation.
Their recommendation: Consider your current technology stack.
You may currently have a vendor in your hospital – like your EHR or virtual sitting provider – that can scale into virtual nursing. This can help to get more ROI out of an investment you’re already making. However, be sure they’re equipped to support you. When selecting a virtual nursing technology vendor, consider the following points:
Platform ease of use: Be sure to select a vendor with a platform that supports multiple clinical use cases and is easy for nurses to use.
Support: There is a lot of clinical change & workflow management that comes with implementing a change to the care model, so select a vendor with expertise who will partner with your clinical teams throughout this process. IT teams also have a lot on their plates and shouldn’t be overburdened with implementing a new platform. Consider a vendor who provides robust technical and project management 24/7 support– not just at the time of deployment, but throughout the partnership.
Demonstrated outcomes: When technology advances, new vendors flood the market. In the clinical space, it’s more important than ever to select a partner with demonstrated experience in delivering outcomes for our patients.
Benefits of a fully integrated virtual nursing program
The promise of virtual care is to create a more sustainable, patient-centered healthcare system that leverages technology to deliver high-quality care anytime, anywhere with greater precision and efficiency. With virtual care workflows as a standard part of care delivery, facilities can meet the evolving needs of both patients & healthcare providers by expanding access to care, improving patient experience, reducing caregiver workload, and increasing the efficiency and scalability of staffing. The path to virtual care maturity requires more than just investing in new technology – it also requires organizational alignment, tight change management processes, and buy-in at all levels of the organization. Adopting an intelligent platform that seamlessly blends remote and in-person care with AI-powered virtual nursing is a critical step towards accelerating virtual care maturity.
The integration of virtual care and artificial intelligence (AI) into the standard care delivery model is permanently reshaping nursing practice. This leads to the pivotal question: How do we best prepare the next generation of nurses to thrive in this environment?
Let’s discuss how innovative technologies are being integrated into nursing curricula, the transition from education to clinical practice, and leadership strategies to foster resilience and innovation within nursing teams.
How to integrate innovative technologies into nursing criteria
It’s no longer optional for academic institutions to adapt to the rise of virtual care, it’s a necessity. Universities such as Chamberlain University, the nation’s largest nursing school, have implemented virtual nursing courses and certifications to better prepare students for the new care delivery model they’ll see in practice. President of Chamberlain University, Dr. Karen Cox, confirms that the traditional nursing education model needs to evolve rapidly to incorporate digital competencies, ensuring that new graduates are proficient in virtual patient care technologies.
What should nursing education institutions do today?
Shift nursing curricula to include AI and virtual care competencies
Provide opportunities for students to gain hands-on experience with telehealth platforms and remote monitoring
Be flexible and responsive to technological advancements
“Chamberlain’s approach allows us to be more nimble compared to traditional academic settings, ensuring students are prepared for real-world challenges.” – Dr. Karen Cox
The importance of supporting new nurses in the transition to practice
The transition from school to practice is a critical time for new nurses, and health care organizations like Community Health Systems (CHS) are integrating virtual care into their onboarding programs. Karen Henson, Corporate Vice President of Nursing Operations at CHS, suggests that facilities build virtual care competencies from day one. Workforce challenges today differ significantly from those a decade ago and organizations need to be adaptable to survive.
Key tips for healthcare institutions:
Embed virtual care training into new nurse onboarding
Prioritize nurse retention by implementing strategies that better support early-career nurses.
Add virtual care programs, presenting an opportunity to bridge workforce gaps and enhance patient safety
“The challenges facing new grads today—like adapting to technology-driven care models—were not issues 5-10 years ago. We have to ensure they feel supported and competent in this new environment.” – Karen Henson
The Role of Nurse Leaders in Driving Change
As virtual care adoption grows, nurse leaders play a pivotal role in shaping policy, accreditation, and workplace culture. Cole Edmonson, CEO of the Nurses on Boards Coalition, emphasizes the importance of leadership advocacy in removing barriers to virtual care implementation. From influencing accreditation standards to creating supportive environments for new nurses, nurse leaders must actively participate in shaping the future of nursing.
Tips for nurse leaders:
Advocate for policy changes that support virtual care transitions
Work to develop a strong culture of mentorship and support, this is crucial for the success of new nurses. Using virtual technology can help overcome the resource gap preventing the same level of preceptorship from pre-pandemic times
Foster collaboration between academia and healthcare organizations to ensure smoother transitions from education to practice.
“Accreditation standards must evolve alongside nursing practice. Leaders have a responsibility to push for policies that facilitate, rather than hinder, virtual care adoption.” – Cole Edmonson
Shaping the Future of Nursing
Nursing leaders, educators and healthcare organizations must collaborate in preparing the next generation of nurses for an AI-driven, virtual care-centric future. As healthcare continues to evolve, fostering a tech-savvy, adaptable nursing workforce will be essential for ensuring high-quality patient care.
Institutions must integrate virtual care and AI into nursing education
Healthcare organizations should support new nurses with robust transition programs
Nurse leaders must play a key role in driving policy changes and cultural shifts in healthcare
AvaSure is committed to keeping this important conversation going, that’s why we create a community of virtual care leaders and bring them together to discuss the pressing issues of healthcare transformation.
As hospitals and healthcare providers face increasing pressures to do more with less, nurses are feeling burnt out. A more novice nurse workforce, in addition to inadequate education and training, higher patient acuity, and rising nurse-to-patient ratios are amplifying this, ultimately leading to nurse staffing shortages. These problems not only affect the well-being of nurses but also impact the quality of patient care.
To address these ongoing issues, hospital systems are reevaluating their workflows and looking at technology solutions to help support their staff. For example, many hospitals are adopting virtual care platforms and AI-enabled tools to help relieve administrative burden. However, before making decisions on solutions, it’s important to really understand the root causes of nurse staffing issues.
Top Reasons for Nursing Shortages:
Nurse Burnout
Nurse burnout is a common consequence of the overwhelming responsibility and pressure placed on nursing staff in hospital systems. Reduced resources and support lead to some nurses deciding to leave the healthcare industry all together. Nurses play a vital role in ensuring that patients’ well-being remains a priority. RNs aren’t the only ones affected; when it comes to Patient Care Technicians (PCTs) and Certified Nursing Assistants (CNAs), health systems are seeing turnover rates in excess of 30%. So, what happens when nurses experience burnout and leave the profession? The remaining nurses within the hospital are stretched too thin with the number of patients they must care for. Job satisfaction begins to decrease, and turnover rates rise, leading to more resources and funds spent to replace and train new staff. As a result, trust in the hospital system starts to fade.
Higher Patient Acuity and Reduced Resources
Another key contributor to the nurse shortage is higher patient acuity and limited training and resources. Patient acuity refers to the level of care or monitoring a patient requires from hospital staff, particularly nurses. The higher the patient’s acuity, the more attention the patient needs. As the patient-to-nurse ratio increases, less attention is given to patients with less demanding issues and health concerns. This leads to diminished patient care, as nurses are unable to provide the attention each patient deserves. Inadequate resources and training leave nurses feeling overwhelmed, making it challenging to provide proper care for all their patients. More experienced nurses are retiring early, leaving junior nurses with a larger workload and less mentorship. This results in stressful situations and higher risk of incidents under the care of the hospital.
Solutions to the Nurse Staffing Shortage
One solution to this issue is to hire additional staff and nurses at the bedside. However, the high cost of hiring travel nurses makes it challenging for hospitals to support their existing nursing staff while meeting the demand for additional help. This is where virtual care can play a key role in providing support, helping optimize the staffing they have. It is crucial for hospital systems to address nurse staffing problems. By providing a better work environment for nurses and offering education and support to nurses’ journeys, hospitals can help the 52% of the nursing workforce who have considered leaving the bedside.
Virtual Care: a Solution to Help the Staffing Crisis
Virtual care is a resource used by healthcare providers and hospital systems to connect patients with doctors, nurses, specialists, and virtual sitting staff remotely. This includes use-cases such as virtual sitting, virtual nursing, and virtual visits. This approach increases efficiency in managing workloads and can help patients receive care more quickly. Virtual care is becoming a prominent resource to help solve staffing issues. It allows nurses to return to the bedside and focus on direct patient care, working at the top of their license. Studies have proven that virtual care, specifically virtual sitting, reduces burnout and improves nurse well-being. A recent survey of 74 nurses from Renton, Washington-based Providence found virtual sitting improved their “emotional labor” and “emotional exhaustion” over in-person sitting. The survey illustrated that virtual sitting improves the well-being of nurses and helps maintain patient safety. Emily Anderson, MSN, RN, PCCN-K, nurse manager at Providence Medical Center in Anchorage, AK said, “Having insightful research into virtual sitting helps us alleviate burnout among our nursing staff and optimize the usage of all our resources to get the right care to the right patient at the right time.” As healthcare systems are evaluating ways to reduce nursing shortages, aid their teams, and deliver the best care possible, solutions like virtual sitting, virtual nursing, and AI need to be considered to support staff and ease the workload and pressure that has been causing the drop in workforce.
What is Virtual Sitting?
Virtual sitting, also referred to as virtual monitoring, is a resource for nurses at the bedside, reducing the need for one-to-one in-person sitting and helping to prevent adverse events for patients. Virtual sitting equips trained safety attendants to use video and audio connections to watch over multiple patients and improve overall safety. Virtual sitting has been used for preventing a variety of adverse events, such as falls, elopement, possible self-harm, suicide ideation, and staff abuse. By using this technology, events that once required 1:1 sitting can now be monitored by a virtual safety attendant, who can safely observe up to 36 patients at a time. This helps reduce the workload of nurses, allowing them to work at the top of their license and focus on higher-acuity patients.
One hospital that successfully implemented virtual sitting amid nurse staffing shortages is St. Luke’s Duluth, a Minnesota-based health system. Like many health systems, St. Luke’s faced challenges such as a tightening labor market, increasing competition for experienced healthcare workers, and rising costs. To provide additional resources and support to their current patient care staff, St. Luke’s implemented a virtual sitting program. They utilize a two-person model: one staff member provides rounding services for patients and staff, while the other staff member observes patients via video monitors. Nursing leaders have found that this approach enhances patient and staff safety and helps support monitoring staff by providing adequate breaks to avoid monitor fatigue.
Another way virtual care has emerged as a solution to nurse staffing problems is through virtual nursing. The American Nursing Association describes virtual nursing as a resource that “support(s) the team at the bedside to alleviate the workload and provide greater satisfaction for both the patients and the nursing staff.”1 Through virtual platforms, nurses and care managers can support teams at the bedside to educate patients, complete admissions and discharge paperwork, automate documentation, and mentor more novice nurses. This allows virtual nurses to have direct, uninterrupted time with patients, leading to less errors or gaps in documentation and freeing up floor nurses to care for their patients at the bedside. It enables a care model where RNs, CNAs, and VRNs (virtual nurses) perform the most appropriate patient care activities based on their skills and experience.
Virtual nursing tools also connect hospital staff with external care providers in real time, ensuring smooth transitions and avoiding delays in securing post-discharge services. Holzer Health System is a recent example of this use case. Using the AvaSure virtual care platform, scarce specialists in neurology, nephrology, diabetes education, and wound care were able to serve patients in two facilities, located 30 miles apart. Natalie Gardner, BSN, RN, CWON, CFCS, describes the benefits: “This has provided a way for me to do video consults with the Jackson facility which saves precious time as well as mileage. The staff take the device to the patient’s room, remove their dressings, and position the patient so that I can see the wound. This leaves me more time to spend with all patients by eliminating the time it would take to drive to Jackson and back.”
Additionally, virtual nurses can provide real-time mentorship, feedback, and confidence to recent graduates and novice bedside nurses, nurturing a nursing workforce for the future.
What is Computer Vision and AI?
While AI is advancing and gaining attention in the healthcare industry, hospital leaders must remember to use applications that can be easily used by their staff, enhance patient safety, and improve the overall hospital experience, all while ensuring that workflow is not disrupted.
There are multiple types of AI currently being used in healthcare settings. Computer vision is a subset of AI that can vastly improve the way hospitals provide care without requiring care providers to compromise on safety and control. One application of computer vision is to help to prevent falls, elopement, and workplace violence by being able to detect factors that are potential warning signs. Following the detection, computer vision alerts a worker to address the issue that may be at hand. The technology is used to augment virtual sitting, helping care team members monitor patients more efficiently, identify patients in need, and make fast, informed decisions that keep them safe.
To know you are using computer vision and AI correctly, keep an eye out for three positive indicators:
Data is used both to prevent immediate incidents and to drive proactive interventions based on insights over time
Real-time alerts are targeted enough to inform the right staff of risk without contributing to alarm fatigue
The program is scalable; AI isn’t just another expense but a way to reduce operational costs and drive savings that fund additional technology investments.
AI in healthcare systems can be a tool but be sure to use the correct collaborative platforms, and track ROI from the start of the AI journey.
A new example of AI in the healthcare space is AvaSure’s virtual care assistant, designed to bridge gaps in communication, prioritize urgent patient needs, and support healthcare teams in delivering timely, high-quality care. The Virtual Care Assistant appears as an avatar, helping triage requests, questions, or needs and assist within the nursing workflow. Requests are categorized into clinical and operational groups, and the assistant, named Vicky, ensures they are directed to the appropriate human personnel or team, helping healthcare systems integrate a reliable, trustworthy, and supportive system for healthcare workers.
Implementing Virtual Care
While there are many virtual care tools and technologies to help reduce the burden on nurses, what does implementation look like in practice? There are multiple phases of the virtual care journey; while it may feel like other hospitals are ahead of the curve, 29% of healthcare leaders established that they have no virtual care solutions, and 39% of hospitals are still in early exploration with virtual nursing. The 5-stage maturity model, developed with the input of 1,100 hospitals and 15+ clinical and hospital IT executives, represents a blueprint for care model redesign led by change-management oriented, outcome-focused leaders. By making virtual care workflows a standard part of care delivery, facilities can meet the evolving needs of both patients and healthcare providers. It can help by expanding access to care, improving patient experience, reducing caregiver workload, and increasing the efficiency and scalability of staffing.
Nurse staffing shortages are a real challenge in hospitals and create a chain reaction that impacts everything, from quality of patient care to the health and well-being of nurses. This issue contributes to burnout and stress, ultimately affecting the care that patients receive. It’s crucial that hospitals find solutions that support nurses and improve the entire healthcare system.
AvaSure’s virtual care platform deploys AI-powered virtual sitting and virtual nursing solutions, meets the highest enterprise IT standards, and drives measurable outcomes with support from care experts. By offering our virtual care platform to monitor and support staff and patients, AvaSure can help reduce the burden on nurses, improve patient outcomes, and assist healthcare systems to better improve staff workflow and patient care.
Resources
1Ball, J. (2022, July 1). Virtual nursing: What is it?. Innovation Site. https://www.nursingworld.org/practice-policy/innovation/blog/virtual-nursing-what-is-it/
These were some takeaways from our most popular session at Symposium 2024! The live session highlighted Regina Foley, EVP and Chief Nurse Executive at Hackensack Meridian Health, and Dr. Nick Patel, CEO of Stealth Consulting, highlighting how clinical & IT teams can partner together.
Virtual care is rapidly changing the healthcare landscape, offering innovative solutions to age-old challenges. But successful implementation requires a strong partnership between IT and clinical leaders.
Two healthcare leaders who exemplify the gold standard of this partnership are Regina Foley, EVP and Chief Nurse Executive at Hackensack Meridian Health, and Dr. Nick Patel, CEO of Stealth Consulting.
Here are five of their recommended best practices for seamless collaboration:
1. Start with the Clinical Need, Not the Technology:
Define the problem: What are you trying to solve? Is it nurse burnout, patient satisfaction, or access to care?
Focus on solutions: How can virtual care programs improve workflows, reduce administrative burdens, and enhance patient care?
Avoid the “shiny object” syndrome: Don’t get distracted by the latest gadgets. Choose technology that truly addresses your needs.
2. Foster a Culture of Collaboration and Trust:
Leave egos at the door: Encourage open communication and mutual respect between IT and clinical teams.
Build a shared virtual care vision: Ensure both teams understand the goals and are working towards the same outcomes.
Involve clinicians in the process: Ensure their input is valued and incorporated into decision-making for implementation of virtual care programs.
4. Prioritize Training and Education:
Provide comprehensive training: Ensure both IT and clinical staff are comfortable using and supporting new technologies.
Offer ongoing support: Address questions, concerns, and challenges that arise during implementation.
Foster a culture of continuous learning: Encourage both teams to stay up-to-date on the latest advancements in virtual care.
5. Embrace AI Cautiously and Strategically:
Focus on data quality: Ensure your data is accurate, complete, and unbiased before implementing AI solutions.
Start with specific use cases: Prioritize areas where AI can have the greatest impact, such as clinical documentation and decision support.
Involve clinicians in AI development: Ensure their expertise is incorporated into the design and implementation of AI algorithms.
Bonus Tip: Don’t be afraid to learn from others! Network with colleagues, attend conferences, and share best practices to accelerate your virtual care program.
By following these guidelines, IT and clinical leaders can forge a powerful partnership that drives innovation, improves patient outcomes, and transforms the future of healthcare.
Interested in more content like this? Save the date for AvaSure Symposium 2025! Registration isn’t open yet, but stay tuned & take a look at our 2024 recap video from attendees.
Falls among VA hospitalized patients are a serious concern and can lead to injuries and increased healthcare costs, often requiring additional treatment and prolonged hospital stays. A recent 8-hospital analysis of over 10,000 patients falls cited by JAMA showed that a fall with any injury is associated with a cost increase of $36,776 and doubles the length of stay.
In VA hospitals, where patients often have more chronic conditions that contribute to a greater falls risk, prevention is critical. Staffing shortages, particularly among Patient Care Technicians and Certified Nursing Assistants, have exacerbated patient safety concerns, with patient falls rising 253% from 2020 to 2022.1 In response, the Veterans Health Administration introduced the SAFE STEPS for Veterans Act in 2024, creating an Office of Falls Prevention.
Addressing Patient Safety Challenges
Facing labor shortages and escalating costs, VA hospitals across the country have turned to virtual sitting, a replacement for traditional one-to-one sitting. Virtual sitting reduces the need for 1:1 sitting by 75% or more, freeing up clinician’s time and headspace for other valuable work.
With AvaSure’s virtual care platform for virtual sitting, a Virtual Safety Attendant (VSA) can oversee up to 16 veterans at once, using an intelligent, AI-enabled platform to identify patients at risk of a fall and verbally redirect them back to safety. If necessary, the VSA can issue a stat alarm, a loud, in-room alarm that draws nearby caregivers to the room in an emergency with an average response time of 20 seconds2. Freeing up CNAs and nurses from one-to-one sitting allows them to move back to the bedside for more direct patient care activities.
An important aspect of virtual sitting is assessing patients individually to determine whether virtual sitting will meet their needs. Conditions typically monitored by virtual sitters include general safety concerns, such as high fall risk, drug or alcohol withdrawal, confusion, agitation, and elopement risk, and failure to follow safety instructions, such as leaving the unit without notifying staff.
Success Stories in Virtual Sitting Implementation for VA Fall Prevention
AvaSure’s virtual care platform is implemented in 45 VA hospitals across the country. For more success stories, check out the whitepaper on VA Fall Prevention.
Fayetteville VA Hospitals
Fayetteville VA hospitals were recently recognized with the 2024 VA Excellence Award when their virtual care program soared to 80% utilization in just six months, highlighting their strong leadership, organization, and commitment to success. Their journey serves as an inspiring model for other VA facilities, proving that with the right strategies and dedication, significant progress can be achieved in a short time.
VA North Texas
Facing labor shortages and escalating costs, VA North Texas implemented a virtual sitting program. At the heart of the program is a centralized monitoring hub, allowing 4 virtual safety attendants to oversee a total of 48 patients to reduce falls.
Since implementing the program, VA North Texas freed up bedside care teams for direct patient care and decreased 1:1 sitter usage, saving the program an average of 83 full-time equivalents per month – an annual savings of $3.4 million. The efficiency gains are substantial, with costs per virtual sitting hour reduced to $3.05 compared to $26 for one-to-one sitters. VA fall rates plummeted by nearly 20%, well below national averages. Learn more about VA North Texas Program
For health systems, one-to-one sitters represent a costly drain on resources that do little to improve patient safety. With virtual sitting, health systems such as VA’s have prioritized fall prevention and created better patient outcomes while delivering staff cost savings that can be invested back into direct patient care.
AvaSure’s Intelligent Virtual Care Platform is deployed in 45 VA hospitals across the country, helping make significant strides in VA fall prevention and patient safety. By leveraging technology and data-driven insights, these hospitals are creating a safer environment for veterans and their caregivers.
By Lisbeth Votruba, MSN, RN, Chief Clinical Officer
The Goal: • Improve patient safety • Reduce fall risk • Increase access to specialty care • Free up CNA and bedside nurses for other activities
The Results: 1. Success of the virtual sitting program: • Saved costs • Improved patient and staff satisfaction 2. Progression into virtual nursing: • Utilization of the same technology • Further cost savings • Enhanced patient and staff satisfaction
Nursing shortages and associated costs are not going away. While RN turnover has dropped from 22.5% in 2022 to 18.4% in 2023, the turnover rate for nursing assistants increased from 33.7% to 41.8% in the same period. And the ongoing costs as nurses continue to leave the profession are high. Each RN that leaves costs an average hospital $56,350, totaling roughly $4M – $6M per year, according to the 2024 NSI National Health Care Retention and RN Staffing Report. Bottom line: nurses need sustained support or the profession will continue to decline in well-being and in numbers.
These challenges hit particularly hard in smaller, community-based organizations. Holzer Health System is a not-for-profit, multi-disciplinary regional health system that provides the full continuum of care for its communities with locations throughout southeastern Ohio and western West Virginia. The system includes two hospital locations, including a rural critical access hospital, as well as multiple clinical locations, long-term care entities, and more than 180 providers in more than 30 medical specialties.
Matthew L. Hemphill MSN, RN, CNML, Director of Acute Care Nursing at Holzer Health System, described the problem: “We want to keep as many of our patients here rather than transferring them out to the nearest tertiary center two hours away. While we did have a small pool of one-to-one sitters, staffing was a challenge. Many needs were going unmet. There were numerous patients who required more monitoring than we could offer.”
Improving care, beginning with virtual sitting
The COVID-19 pandemic made matters worse, so Holzer had to come up with a workable plan that would allow it to augment its existing staff while keeping a larger volume of patients safe.
Holzer undertook a major initiative to improve patient safety, reduce fall risk and increase access to specialty care by securing a grant through the FCC COVID-19 Telehealth Program to implement an inpatient virtual sitting solution.
With the aid of the grant, Holzer implemented AvaSure’s virtual care technology to support virtual sitters, who watch over patients via video-and-audio connections to enhance patient safety, such as reducing patient falls and elopement. The health system implemented 16 devices, including four ceiling-mounted devices, 12 mobile devices and a centralized monitoring station. The primary goal was to enable and expand the use of virtual sitters, freeing up CNAs and bedside nurses for other care activities.
After seeing the virtual sitting program’s success in saving costs, as well as improving patient and staff satisfaction, the health system progressed into virtual nursing using the same technology platform. AvaSure’s intelligent virtual care platform enables virtual sitting, virtual nursing and specialty medical consults.
Progressing to inpatient virtual nursing and realizing multiple improvements
When Holzer progressed from virtual sitting to virtual nursing, one key principle it followed was to structure the use of virtual sitters and nurses so that all nurses work at the top of their licenses. This enables a care model where RNs, CNAs, and VRNs perform the most-appropriate patient care activities based on their skills and experience.
Using the AvaSure platform, scarce specialists in neurology, nephrology, diabetes education and wound care can serve more patients in both facilities, the main Gallipolis Hospital and the rural critical access Jackson Hospital.
For example, Holzer has one certified wound and ostomy nurse (CWON) serving both facilities, located 30 miles apart. Natalie Gardner BSN, RN, CWON, CFCS, described the benefits: “This has provided a way for me to do video consults with the Jackson facility which saves precious time as well as mileage. The staff take the device to the patient’s room, remove their dressings, and position the patient so that I can see the wound. This leaves me more time to spend with all patients by eliminating the time it would take to drive to Jackson and back.” Giving patients easier access to specialists improves care and facilitates early intervention to prevent transfers from the critical access hospital to the main facility.
Continuing to hone the virtual nursing program
For community health systems, the strain on resources will continue for the foreseeable future. Progressing on a path from virtual sitting to virtual nursing extends precious resources to enable high quality patient care, while allowing all nursing staff to work at the top of their skills and licenses. Holzer is continuing its path to expand its virtual nursing program to encompass more activities across more inpatient care units. At every stage, Holzer is delivering better patient outcomes while enabling a care model that gives nurses more time for their most satisfying work – spending time on direct patient care.
Explore their journey of virtual patient monitoring from evaluation to implementation to outcomes, including a significant reduction in falls, zero patient falls with injuries in 2022, and improved staffing efficiencies.
Challenge: Reducing patient falls
CHS, one of the largest provider organizations in the United States, operates across 43 distinct markets in 15 states. Their decade-long commitment to high reliability, safety, and harm reduction aligned perfectly with the need to reduce falls during the pandemic in 2021. Hospitals across the nation have been grappling with staffing shortages, leading to nurse burnout and a rise in adverse patient events. As the personnel issue worsened, many healthcare systems asked: How can hospitals create a care system that reduces the need for 1:1 patient sitters while allowing nurses to focus on critical patient care?
Evaluating solutions: Evidence and scalability
In their quest for the right solution, CHS employs a rigorous evaluation process. Their primary criteria encompass two crucial elements: evidence-based effectiveness and scalability. First and foremost, CHS seeks evidence-backed solutions, emphasizing clinical outcomes and operational impacts. This commitment to data-driven decision-making ensures that any chosen solution delivers tangible benefits across both patient care and operational efficiency.
The second key criterion is scalability. Given CHS’s size, the ability to initially implement a solution at a few select hospitals and then scale it elsewhere across the organization is paramount. In this regard, AvaSure’s TeleSitter solution met these criteria for virtual patient monitoring, making it a natural choice to address their needs.
Phase 1 deployment: Keys to success
CHS’s journey with the AvaSure TeleSitter solution commenced with a pilot deployment at three hospitals and then scaled to 17. This pivotal phase yielded notable success, attributed to several critical factors:
Intentionality: The deployment of virtual patient monitoring was marked by a deliberate and well-thought-out strategy. Every step was carefully considered, from initial planning to execution, ensuring a seamless integration of the TeleSitter solution into their healthcare ecosystem.
Metrics that matter: A key driver of success was CHS’s dedication to data-driven decision-making. They recognized the importance of collecting precise and relevant data to assess the impact of the TeleSitter solution accurately. This commitment to meaningful metrics allowed them to track progress, identify areas for improvement, and ultimately optimize patient care outcomes.
Leadership and oversight: Strong leadership and dedicated oversight were pivotal throughout the deployment process. Key leaders within CHS played a central role in driving the virtual patient monitoring initiative forward. Their unwavering commitment and guidance ensured that the program remained aligned with the organization’s broader goals and objectives.
Buy-in and Teamwork: CHS understood that achieving the desired results required a collaborative effort. Encouraging buy-in and utilization among staff was essential. Through effective communication, collaboration, and trust, the healthcare team worked together to maximize the benefits of the TeleSitter solution. It became a team effort, with everyone playing a crucial role in its success.
Strategic Patient Selection: CHS recognized the importance of strategic patient selection in applying the technology where it would be most effective. Careful consideration was given to identifying patients who would benefit most from the TeleSitter solution, further optimizing its impact on patient safety and care quality.
This comprehensive approach to the Phase 1 deployment set the stage for CHS’s journey implementing virtual patient monitoring, paving the way for positive clinical and operational results.
Outcomes: Reduction in falls and positive operational and financial impact
Following the completion of the pilot program, CHS embarked on a thorough analysis, which unveiled some significant outcomes.
A Meaningful decrease in falls: While CHS has worked effectively to reduce falls for years, implementation of the TeleSitter solution led to an even greater reduction in falls, including a 76% reduction in one hospital.
Zero patient falls with injuries in 2022: In 2022, CHS reported zero patient falls with injuries at facilities using virtual patient monitoring. This milestone reflects a profound commitment to patient safety.
Savings through injury avoidance: The solution translated into meaningful savings through the avoidance of costs related to patient injuries. In an environment where litigation looms, AvaSure can help mitigate potential liability claims when it comes to falls with injury.
Staffing dfficiencies of 16 to 1: The introduction of virtual sitters had a strong effect on staffing efficiency. With each virtual sitter capable of monitoring up to 16 patients simultaneously, CHS achieved staffing efficiencies of 16 to 1. This efficiency not only optimized staffing allocation but also enabled caregivers in CHS hospitals to work at the top of their licenses and provide more attentive care to a broader patient population.
These outcomes are a testament to CHS’s commitment to excellence, safety, and innovation. AvaSure delivered quantifiable operational benefit and helped reinforce the high standard of patient care and safety across CHS.
Quality and patient care lead to next steps
Today, CHS is poised to expand virtual patient monitoring services. With 87 devices currently in place, CHS plans to add78 more across 12 more hospitals by the end of 2023.
CHS’s innovative approach helps ensure that more patients are kept safe, more healthcare professionals are supported, and the future of healthcare is brighter than ever.
Watch the webinar replay to hear firsthand from CHS about how they expanded their virtual patient monitoring program to enhance patient safety and optimize resource utilization.
Today, CHS is poised to expand virtual patient monitoring services. With 87 devices currently in place, CHS plans to add 78 more across 12 more hospitals by the end of 2023.