Background: Although video monitoring has been shown to reduce falls among at-risk hospitalized patients, there are no identified best practices for the monitoring process.
Purpose: The purpose of this study was to evaluate the monitoring process at a large teaching hospital, with the goal of making improvements and standardizing monitoring practices.
Methods: Patients and nursing staff perceptions about the video monitoring process were elicited via survey, and perceptions of monitor technicians were obtained through structured interview.
Results: Video monitoring was perceived by all groups as effective in promoting patient safety. Nursing staff and monitor technicians also indicated that monitoring protects patient safety in other high-risk situations. Suggestions for improvement and standardization in the monitoring process were made by study participants.
Conclusions: Suggested changes and standardization of the monitoring process have been implemented in the study facility. Insights are provided for other facilities considering video monitoring for patient safety.
Patients receive mixed messages—try to be as independent as possible, but don’t do anything in your room without calling for assistance. Falls are a significant issue in rehabilitation settings. Patients are encouraged to be as independent as possible, yet not to do anything without assistance. This mixed message leads to the increased risk for falls in this setting.
Solution
Video monitoring significantly lowers the risk of falls. The focus of this project was on a 31-bed brain injury unit of an inpatient rehabilitation facility where the majority of falls occurred. Fifteen video monitoring units were installed and total falls and falls rates were tracked.
With video monitoring:
The average number of falls was decreased to 6.87 falls per 1000 patient-days compared with 10.26 falls per 1000 patient-days before video monitoring was implemented. This is a statistically significant improvement
There were 32 fewer falls in a 1-year period
There was a reduction in costs due to falls and fall-related injuries of at least $40,000 —this sum is thought to be a conservative estimate
The hospital saved nearly $190,000 on the cost of 1:1 sitters
Total costs for the video monitoring system were recouped in 12 months of continued use
Staff response to the video monitoring system has been strongly favorable.
81% of respondents indicated either a generally or strongly favorable reaction to the video monitors
Nearly all respondents—96%—felt that video monitoring did not intrude on privacy
Conclusions
Video monitoring can provide greater safety for patients by decreasing falls. Additionally, video monitoring decreases sitter usage and its cost, and enhances satisfaction.
ALBANY — The Phoebe Putney Memorial Hospital Board of Directors got its first look Wednesday at a new piece of technology meant to help prevent patient falls.
The AvaSys Telesitter® program, which has 12 units between the main hospital and Phoebe North, works by putting more eyes on patients.
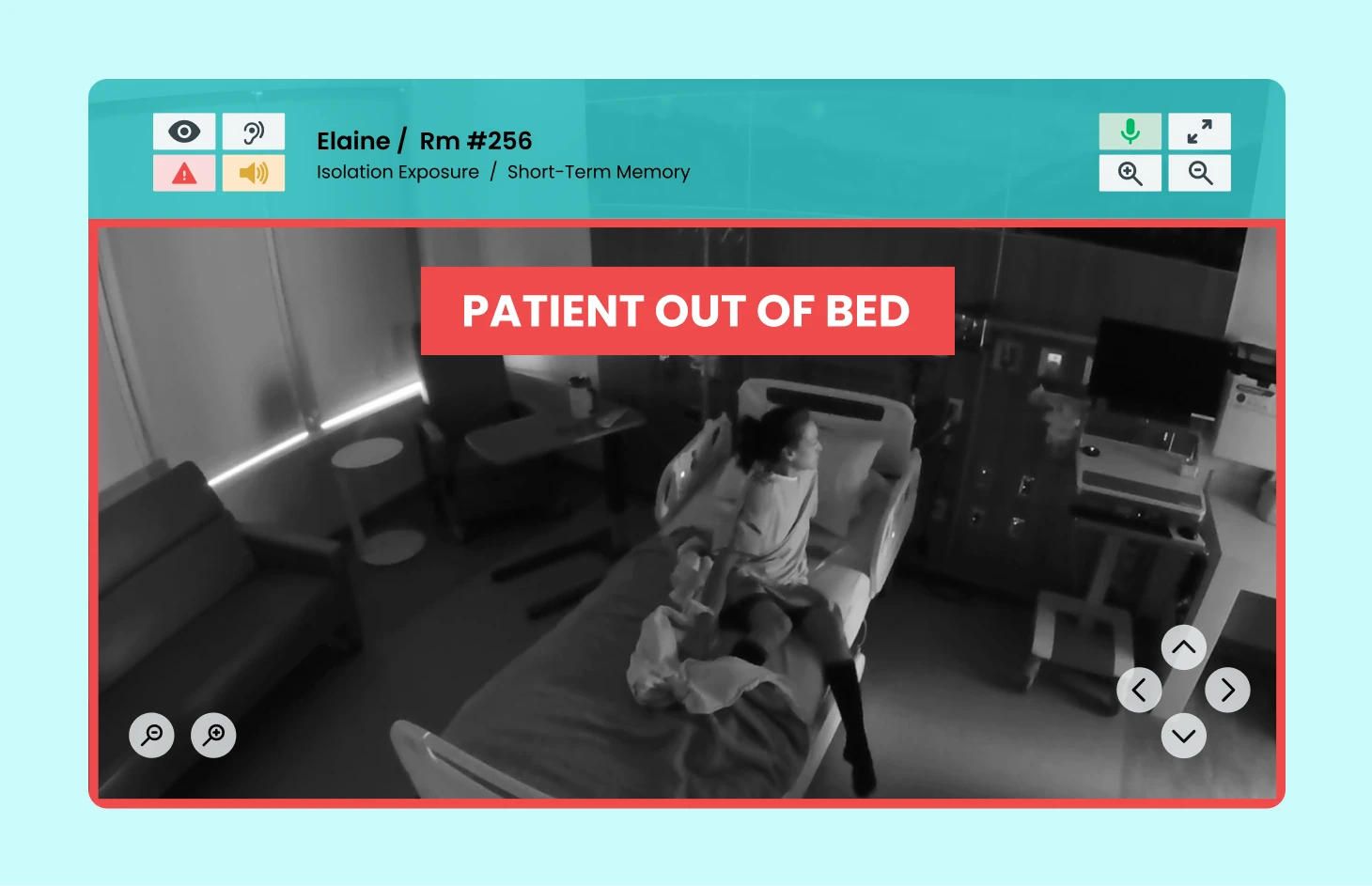
Equipped with an infrared camera and two-way audio, it is set up in rooms of patients identified as high risk for falls. One technician can monitor live feeds on the units from those rooms at a central station.
If a patient tries to get out of bed, the observer can interact with the patient with a reminder to wait for assistance or sound an alarm for immediate staff attention. Patients in imminent danger receive an alarm, which signals the staff to head quickly to the patient’s room.
“Within seconds, someone is in the room,” April Little, a central staff manager for Phoebe Putney Health System, said of the alarm.
Caring for patients with increased safety needs and those needing 1:1 observation is a challenge to hospital resources. One of the most expensive safety practices in acute care hospitals in the United States is the use of constant observation. Most programs are developed with patient safety in mind, but the costs increase over time.
What’s more, the literature on constant observation shows very little proof of improvement in successful outcomes, such as fewer falls.
Solution
Clinical Nurse Specialists identified 8 units for a pilot program using video monitoring. During the 3 quarters following the implementation of video monitoring, there was a significant impact on resource utilization. With the use of full-time patient safety attendants, there was an approximate annual savings of $211,000 and no increase in the number of falls.
Posted on August 21, 2017 by Olivia Phillips - Uncategorized
LAKE CHARLES, LA (KPLC) – Patient safety is paramount in hospital settings and traditionally, it has taken one-to-one care 24 hours a day for some of the most at-risk patients.
That can tie up skilled nursing staff from other demands and that is why a new video monitoring system has been launched at Lake Charles Memorial Hospital.
It is called the AvaSure Telesitter® Solution and through a two-way audio system, video camera, and central monitoring station, Memorial nurse manager, Tressy Bergeron, is able to keep an eye and ear on up to 12 patients at one time.
In-hospital safety sitters are associated with a range of disadvantages. Safety monitors are a valuable resource in maintaining patient safety. Yet, there are limitations:
They are typically used in hospitals to directly observe 1 to 2 patients to prevent patients from falling or injuring themselves.
As a resource, they are not always available to nursing staff due to the difficulty in predicting when they are needed.
Their use increases the costs of delivering care.
Hence, this frequently results in acquiring per diem staff or reassigning staff to monitor fall risk patients. Such alterations in staffing can lead to job dissatisfaction.
Solution
Remote Video Monitoring with AvaSure. Remote video monitoring provides a live-stream video of patient activity as an additional safety intervention in preventing falls.
This technology provides an innovative fall prevention strategy that allows the sitter to monitor multiple patients at one time.
It is important to keep in mind that sitters require training to use the software functions, such as navigating the camera and alert options, and have the confidence needed to verbally intervene when they recognize unsafe patient behaviors. Additionally, the remote sitter must be able to multitask, such as demonstrating competencies using the PC while monitoring the television screen, allowing them to visualize each of the patients being monitored.
While remote video monitoring may not completely end patient falls, it is an additional resource that can be used in the clinical arsenal of fall interventions—and having an extra set of eyes to monitor patient activity is always helpful.
Conclusions
This technology provides an innovative fall prevention strategy that can improve fall-related patient outcomes and sitter costs.
With increasing acuity and simultaneous pressures for optimal productivity, reducing unnecessary patient companions has been a focus for many health care organizations. At the same time, nursing leaders are seeking to accelerate improvement in patient safety, specifically the prevention of falls. This study suggests the use of remote video monitoring is a safe tool for fall prevention. While there was a decrease in 1:1 sitter usage, there was no corollary increase in falls. In fact, falls decreased 35%. Not only was video monitoring a safe intervention, it was more effective than patient companions alone in decreasing falls by expanding the number of patients who are directly observed 24/7.
Sitters are a variable staffing resource that can be difficult to predict and accurately budget. Given multiple pressures to reduce self-injury from falls and other high-risk safety concerns, such as pulling tubes and lines, elopement risk, and suicide risk, the UC San Diego Health System (UCSDHS) implemented a patient sitter program. Sitters were used to closely observe 1 or more patients in direct line of sight. Yet, the costs of these sitters continued to rise.
Annual sitter costs in 2012 were estimated to be $3,197,515 across both UCSDHS locations
Therefore, nursing leaders initiated an evaluation of the sitter program with the aim of recommending and implementing new technologies or changes in current practice that would maintain or improve patient safety while reducing costs of care.
Solution
Goals for the video monitoring project included reducing sitter costs and outperforming national benchmarks and nursing-sensitive indicators (falls, falls with injury, and restraints).
In the first year (9 of 12 months implementation), there was a 24% reduction in combined video monitor technician and sitter staffing, for an estimated savings of $771,919
In the second year, the program realized a 54% reduction in staffing, for an estimated savings of $1,718,823
The return on investment for these units alone was 8.9 times the initial investment (calculated based on combined costs for video monitor technician and sitter staffing)
26% (average) reduction in falls with injury—outperforming or equaling benchmarks per 1000 patient days
Conclusion
The UCSDHS experience has demonstrated that nursing culture can shift and trust in the effectiveness of a new technology to address patient safety, such as video monitoring.