Hear from nurse leaders at a children’s hospital and an acute-care hospital on how remote safety monitoring has succeeded in reducing adverse events for pediatric and adolescent patients.
Caring for children in the inpatient setting presents unique challenges. Like adults, kids can misuse medication devices, elope from the hospital and sustain injuries from falls, but their needs are different and require additional attention from nurses. More than ever, young patients have behavioral health problems ranging from eating disorders to major depressive episodes, a situation made worse by the pandemic. Providing one-to-one care for this patient cohort is costly, ineffective, and resource intensive.
Hear from nurse leaders at a children’s hospital and an acute-care hospital on how remote safety monitoring has succeeded in reducing adverse events for pediatric and adolescent patients while reducing stress on families and caregivers.
Presenters:
Jamie Clendenin, BSN, RN-BC, Supervisor, Nursing Operations, Anne Arundel
Melanie Lee, MSN, RN, CPN, Clinical Director, Pediatric Emergency and Inpatient Unit. Anne Arundel
Learn why virtual sitting is a solution to address the top patient concern for 2023 – the pediatric mental health crisis.
Caring for children in the inpatient setting presents unique challenges for hospitals across the nation. Similar to adults, kids can interfere with medical devices, elope from the hospital, and sustain injuries from falls, but their primary needs tend to differ and nurses caring for these patients need different support. Pediatric patients have always required a different touch, but the situation is being exacerbated by persistent staffing shortages and the concurrent mental health crisis amongst young Americans. Youth patients in need of behavioral health services are being kept in the ED due to a lack of mental health facilities and appropriate staffing. This makes providing safe and effective care to this important patient cohort costly, ineffective and resource intensive.
Advances in technology, like virtual sitting, have proven to support adequate staffing and allow children to be safe and well cared for. Hear how nurse leaders at a children’s hospital and an acute-care hospital are using virtual sitting for pediatric and adolescent patients and have succeeded in reducing adverse events while also reducing stress on families and caregivers. In addition, they will discuss the policies and procedures to consider and how to get buy-in from your team for this specific patient population.
Learning objectives
Policies and procedures needed for video-monitoring pediatric patients.
How to get buy-in from your frontline team to use technology for this sensitive patient cohort.
Why virtual sitting is a solution to address the top patient concern for 2023 – the pediatric mental health crisis.
The ins and outs of behavioral health monitoring, including regulatory standards, device selection, patient consent, and evaluation tools in utilizing virtual monitoring for patients at risk of suicide.
Mental health conditions are on the rise in all age groups, affecting millions of Americans. Providing safe care for patients with behavioral health needs can be especially difficult when they are in emergency departments or acute-care settings that are not designed for their needs. Too often, hospitals resort to using costly 1:1 sitters to monitor patients with low-to-moderate suicide risk, and providing this sitter often means pulling a much-needed care staff member from the floor. In a world where hospitals are pressed to “do more with less” this can exacerbate already stretched staffing levels, which is why hospitals are looking for more scalable ways to keep their at-risk patients safe. There is a perception that virtual sitting solutions aren’t allowed or suitable for these patients – in reality, while policies may have to be adjusted, most governing bodies allow for the virtual monitoring of patients that are assessed to be at low and moderate risk of suicide. Using a TeleSitter® program for these behavioral health monitoring can help reduce placing additional staffing constraints on your system while empowering patients on their journey to well-being.
What are the regulatory standards for behavioral health monitoring?
With virtual sitting proven as a reliable solution for preventing falls, the question has naturally risen whether it is a suitable method for monitoring other vulnerable patients, including those at risk of suicide. Research led by David Kroll, MD, of Brigham and Women’s Hospital in Boston, showed that having a 1:1 sitter in the room of a suicidal risk patient is unproven in preventing self-harm. By contrast, use of the TeleSitter® solution on suicide risk patients resulted in zero adverse events.1 This study paved the way for the Joint Commission to deem the use of video monitoring for patients who are not at high risk for suicide up to the discretion of the organization in 2019.
Hospitals in 45 states across the U.S. are using AvaSure to virtually monitor over 75,000 patients for low-to-moderate risk of suicide.2
Do patients need to complete an informed consent form before they can be monitored?
Patient consent is not necessary for non-recorded video monitoring when it is solely employed for the purpose of ensuring patient safety, allowing healthcare providers to promptly implement essential monitoring systems that prioritize patient welfare, and fostering a safer and more secure healthcare environment. AvaSure’s platform does not record videos of patients.
What devices are best for behavioral health monitoring?
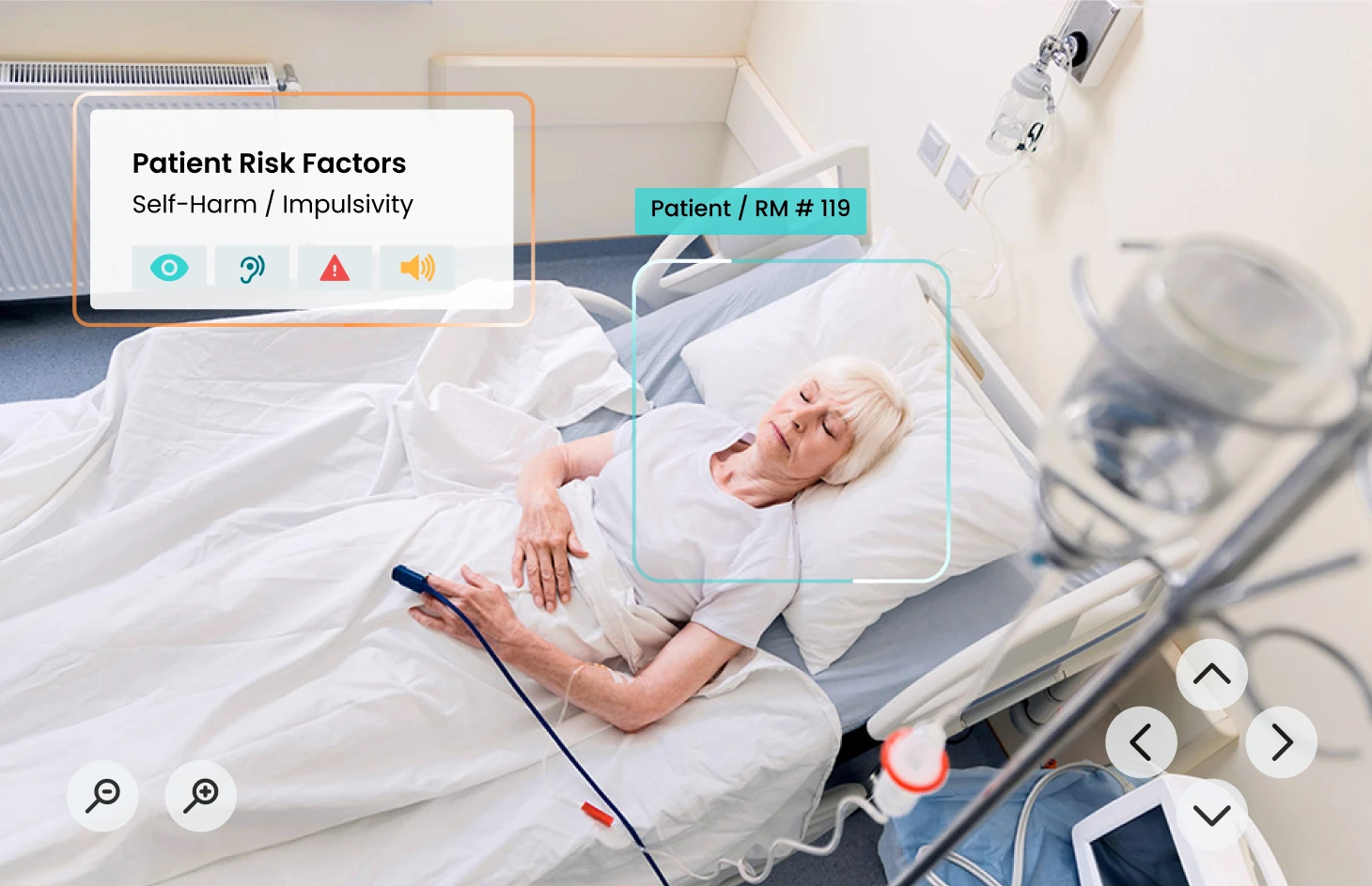
Selecting the right device is key to ensuring patient safety. You will need a robust device that offers 360-degree pan/tilt/zoom functionality for a comprehensive view of the surroundings. The device should feature infrared viewing to ensure visibility during both the day and night. High-resolution capability is essential to enable effective risk assessment, such as identifying potential hazards like trash bags, lines, or hidden items.
Two-way communication capabilities are a must for verbal redirection, especially in situations where a patient may attempt to go into the bathroom alone. And finally, any alerts from the device must be loud so staff can quickly respond to potential safety concerns.
AvaSure offers robust device options suited to meet the needs of behavioral health monitoring, such as patients at risk of suicide, including ligature-free ceiling options.
What tools are used to evaluate patients for suicide risk?
It is up to the discretion of the care team to determine if a patient is appropriate for virtual monitoring based on the hospital’s protocols and clinical judgment.
It’s critical to have an adequate, evidence-based screening tool in place to conduct suicide risk assessments. The Columbia Suicide Severity Risk Scale (C-SSRS) is the most commonly used tool to assess suicide risk, and we highly recommend it. However, if you’re interested in exploring other options, The Suicide Prevention Resource Center provides a variety of resources for different risk stratification tools.
To keep everyone on the same page, it’s important to review and address any existing hospital policies around suicide risk assessments. Depending on the state and other regulatory factors, there may be additional compliance considerations to keep in mind.
At the end of the day, our goal is to work collaboratively with hospitals and providers to ensure that every patient receives the appropriate level of monitoring to keep them safe and healthy. AvaSure’s Customer Success team will advise and help your team develop policies and risk stratification that work best for your hospital and patient population.
How do you overcome adoption challenges in behavioral health monitoring?
Change management is key. It’s common for staff to initially feel hesitant to use a virtual monitoring solution in place of a 1:1 sitter. First and foremost, ensure your staff understands the inclusion and exclusion criteria for patients and the screening process. You’ll want to keep everyone in the loop so they can feel confident about the new system. To make everyone feel even more comfortable, many facilities run pilots where a virtual monitor is used alongside an in-person sitter, who is just outside of the room. This safety net not only eases minds but also proves the efficacy of the system.
And don’t forget to celebrate the good catches! Sharing your successes with hospital leadership, nurse managers, and front-line staff is crucial to building goodwill around your new behavioral health monitoring program and gaining support. AvaSure provides a toolkit for our customers to easily share the good news with their hospital.
Are the staff monitoring for suicide risk required to be clinical or specially trained in any way differently from those monitoring for falls, elopement, etc.?
While there are no formal requirements for specialized training, we highly encourage you to invest in additional training to ensure your staff is fully prepared for their role. We recommend annual education and competency validation for Virtual Safety Attendants (VSAs) along with education on the risk of suicide to ensure that your team’s skills remain sharp while monitoring this vulnerable patient population.
But it doesn’t stop there – it’s equally important to train your bedside staff. By sharing stories and experiences that highlight the potential consequences when things go wrong, you can drive home the need for compliance and create a sense of urgency around proper training.
At AvaSure, we provide specialized training and competency evaluation resources that equip your VSAs with the knowledge and skills needed to effectively monitor patients at risk of suicide. From screening the room for potential safety risks to redirecting patients who may attempt to use the bathroom alone, our training ensures that your VSAs are well-prepared for any situation.
By investing in comprehensive training for your virtual safety attendants and bedside staff, you can enhance the overall safety and well-being of your patients. Together, we can ensure that everyone is equipped with the necessary knowledge and skills to provide the highest level of care.
AvaSure’s Customer Success team is comprised of nurses and change management experts who are ready to guide you through best practices and provide clarity, policy templates, training, and resources about using behavioral health monitoring to keep patients safe. Schedule a discovery session with our team today.
Kroll, D. S. et al., (2020). Virtual monitoring of suicide risk in the general hospital and emergency department. General hospital psychiatry, 63, 33-38. https://doi.org/10.1016/j.genhosppsych.2019.01.002
Insights from AvaSure’s national database on virtual monitoring (ORNA®)
Discover how virtual monitoring for low-to-moderate suicide risk patients can help.
The increasing prevalence of mental health conditions demands innovative approaches to ensure patient safety. Traditional methods like costly 1:1 sitters are unsustainable in the face of labor shortages.
Over 45% of AvaSure’s clients across the country are embracing virtual sitting for low-to-moderate suicide risk patients, and the results speak for themselves. Increased staff satisfaction, decreased 1:1 sitter costs, and better patient outcomes are just a few of the advantages of implementing the TeleSitter solution.
Download our latest use case spotlight to access valuable evidence and proven strategies for virtual sitting for low-to-moderate suicide risk patients.
In this post-pandemic world, we are seeing an uptick in behavioral health patients across the u.s., especially in our vulnerable pediatric population. When we pair this with a shortage of mental health professionals, there is a risk in our ability to adequately care for this important demographic. One particular challenge is handling suicide ideation (si) patients in acute care facilities, as they require a one-to-one sitter for their health and safety.
With our current staffing situation, providing this sitter often means pulling a much-needed member of the care staff off the floor. This can exacerbate already strained staffing, which is why telesitter solutions are so important for low and moderate risk si patients and why AvaSure pulled together this panel for our annual symposium. There is a perception that telesitter solutions aren’t allowed or suitable for these patients – in reality, policies may have to be adjusted, but most governing bodies allow for the virtual monitoring of si patients that are assessed to be low or moderate risk. Using a telesitter program for these patients can help reduce placing additional staffing constraints on your system while keeping patients safe.
Read below for key highlights from our panel discussion on this underutilized but important use case of the telesitter solution:
Q: Why did you first implement a TeleSitter program? Did you consider using it for SI patients at that time?
HCA Methodist & St Peter’s Health both were primarily focused on falls prevention when first building out their programs and the inclusion of use on SI patients came down the road. Both saw challenges increasing where CNAs, RNs, and even administrators were being pulled to sit with patients exacerbating the need for another solution.
Ascension Michigan started the program with SI in mind, but offsetting sitting costs related to patient falls were the driving factor
Q: Was there a perception that TeleSitter solutions couldn’t be used for SI patients & how did you overcome this challenge?
Most hospitals have a policy in place that needs to be addressed & reviewed. In some instances, depending on state legislation, it may be important to include your regulatory/compliance managers as well. Ensure that you have an adequate screening tool in place – most customers on the panel utilized the Columbia suicide screening tool to assess for low/moderate/high risk. This will be important in case of an potential JCO visits that staff is aware that screening does take place before placing a patient on virtual vs. in-person sitting.
As the program gets started, be sure to share good catches with hospital leadership, nurse managers, and front-line staff. This is key to building good will around the program and gaining support.
Once the team understood that the devices do not record & are fully HIPPA compliant, there was no longer a concern about it potentially violating JCO regulations to utilize virtual monitoring
Q: Were there any specific challenges with getting physicians on board?
Some physicians were hesitant at first, especially pediatrics. To help build confidence, multiple facilities conducted a pilot where a video monitor was used in combination with an in-person sitter who sat outside the room. This allowed for a safety net while they proved out the efficacy of the system.
One panelist noted that less than a year into the program, providers don’t hesitate to rely on the TeleSitter staff for monitoring these patients
However, all systems noted you’ll have to stay on top of educating new providers & residents as they join the system – so continue to share great catches even after initial implementation
Q: Are the monitor staff for SI patients required to be clinical or specially trained in any way differently from those monitoring for falls, elopement, etc.?
All the systems on the panel utilize the same monitor staff which can be clinical but are not required to be when monitoring all patients – including SI
The training modules on monitoring Suicide Ideation Patients from AvaSure were viewed by all as an essential tool in training staff to properly monitor this patient population
One panelist recommended the best practice of rotating “on-site” 1:1 sitters and virtual monitors so they have an appreciation for both versions of the program helping to build consistency
Another best practice is that if monitor techs aren’t yet at their maximum number of patients being monitored, consider having multiple monitor techs viewing a SI patient for an extra set of eyes on these patients
In addition to training monitor staff, it’s essential to train bedside staff. Most aren’t adequately educated on the details of their hospital policy regarding sitting & sharing stories of what could happen when things go wrong can help to drive the need for compliance.
Q: What advice do you have for customers just thinking about rolling out a TeleSitter program for monitoring SI patients?
Consider your use cases when selecting devices. Not all TeleSitting devices are ligature free, so if you’re thinking about monitoring SI patients from the onset or down the road, share this with your vendor to ensure you purchase the correct devices
Hold a roundtable with various departments allowing for open conversation between leaders prior to rollout. This can help to identify any areas of concern that you can then be laser focused on addressing.
Don’t underestimate the number of cameras you’ll need – Kim Beckett from Ascension said the program would be easier to manage with a camera in every patient room!
“It’s possible, efficient & effective. The camera prevents harm,” said one panelist while another noted, “don’t hesitate. Education is how you overcome any potential pushback. The results will speak for themselves.”
The team was able to share several great catches, all noting they have not yet had a successful attempt on a patient being monitored by their TeleSitter program. In addition to more typical catches, such as a patient attempting to strangle themselves with heart monitors, they also caught things like a patient who was able to smuggle in materials from the outside & an incident where an on-staff security guard entered a pediatric patient room and was overly aggressive with the patient. Events like this have caused the facilities to think outside the box on future potential use cases for their TeleSitter programs – such as watching infants for potential abduction, monitoring eating disorder patients & keeping an eye on family members in the room for potential staff or patient injury & medication theft. With a well supported program, the use cases truly are endless. If you’d like to learn more about potential use cases, we’d be happy to complete a complimentary on-site assessment and make recommendations.
As the COVID-19 pandemic continues to rage across the country, it is vital that we continue to shine a light on the threats faced by nurses and other frontline health care workers. In fact, more than 1,700 health care workers have died from COVID-19, according to a September 2020 report by National Nurses United. With gaps in tracking and recording, that number may be much higher.
Every day, hospital staff around the country are putting their health and safety on the line to care for sick patients – and it’s having a toll. Medical personnel account for as many as 20% of known coronavirus cases in some states, according to Kaiser Health News. What health care leaders and society as a whole learn in this moment – about how to care for the nurses and frontline workers who care for us – will prove crucial now and in the future.
The evidence for 1:1 observation is lacking and costly. Constant observation of patients who are determined to be at risk for suicide is rooted more deeply in tradition than in research. Yet observation is considered essential for these patients, and failure to do so would be deemed negligent.
Solution
Many patients at risk for suicide can be continuously monitored virtually. In this retrospective analysis at an academic tertiary hospital, 39 patients (27 [69%] on hospital floors and 12 [31%] in the emergency department [ED]) received virtual monitoring over a total of 2318 monitoring hours.
The goal of this analysis was to assess the number of adverse events among patients who received virtual monitoring for suicide risk. It found that no adverse behavioral events were reported among this group of patients.
Conclusions
This study shows that appropriately identified patients who are at risk for suicide can feasibly be monitored in the general hospital and ED settings using virtual monitoring.
Posted on February 27, 2019 by Olivia Phillips - Uncategorized
Beacon Health Memorial Hospital Implements Successful Virtual Sitting Program: Zero Adverse Events Found in Study of 500+ Patients. In a proactive approach, Beacon Health Memorial Hospital assembled a dedicated multi-disciplinary team of frontline staff. This team thoroughly assessed their existing procedures, developed new policies, and implemented a stringent patient selection process using the Columbia Suicide Severity Risk Scale (C-SSRS) for eligibility criteria. Conducting their study across two hospitals and involving over 500 patients, their implementation of the TeleSitter solution yielded impressive results: zero adverse events reported.